Increased erasure. Tooth wear: main symptoms. Types of pathological abrasion of enamel
Oral health is a very pressing issue for many. How beautiful and healthy a person’s teeth look can be used to judge his health, grooming and status. Ecology, stress, neglect of oral problems and non-systematic visits to the doctor contribute to the formation of various dental problems and diseases.
Pathological abrasion of teeth is a pressing problem. This is normal physiological process body. In people who have a correct bite, scratching the tooth enamel of the upper teeth begins with inside, and the lower ones, respectively, outside. The problem may arise when a person reaches a more mature age and develop into a pathological process.
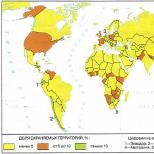
According to the data statistical research, 12% of the world's population is prone to pathological tooth wear (men are at greater risk - 63%). By the age of thirty, a certain layer of enamel is gradually worn away, and after fifty, the wear of the dentin layer is often recorded. If such problems begin to appear at a younger age, we can talk about the pathological nature of this problem.
The main reasons for the appearance

Anatological abrasion of teeth is usually called the systematic abrasion of the enamel (in some cases, enamel and dentin) of all or several teeth. The level of neglect of this process can only be determined by a doctor using basic methods:
- Examination of the jaw model using a cast.
- Electrodiagnostics.
- Electromyography.
- Orthopantography.
Causes of dental pathology
Experts combine the main causes of this anomaly of tooth enamel into two groups, namely:
— Functional deficiency of hard dental tissues:

— Waste of human teeth due to problems associated with:
- loss of teeth (partial);
- bad habits, which very often cause systematic injury to human teeth;
- resulting hypertonicity of the human masticatory muscles (can be formed due to tense facial muscles);
- foodless chewing.
Classifications of increased tooth wear
Classification of this pathological disease compiled depending on the forms and complexity of the disease.
There are main degrees of abrasion:

Taking into account the level of the erase plane, the following types are distinguished:
- Vertical, most often found in patients with malocclusion. Only the outer side of the tooth enamel is erased.
- Horizontal. As teeth wear down, the height of the crown decreases.
- Mixed. When this level of the disease is reached, erasure of the two previous types is characteristic.
Depending on the complexity of the process, they differ:
- local abrasion. In this case, one specific area is subject to erasure;
- generalized. In this case, the process completely affects all areas of a person’s teeth.
To summarize, we can talk about numerous variants of manifestation of this dental pathology, in which all the enamel can be completely erased or only some part of it, one side - or both at once.
Symptoms of the disease
The symptoms of this disease depend both on the degree of the disease and on its course.
It's broken from the start primary view teeth. If measures are not taken, the disease develops, causing the length of the tooth to become much shorter than before. The chewing function of a person is impaired. Patients note discomfort when taking hot, cold, sweet or sour food, which indicates the onset of hyperesthesia.

Impaired chewing function is a sign of a disease called increased tooth wear. Tooth enamel is about five times stronger than dentin, therefore, until the enamel is completely erased, the symptoms are mild, but as soon as the enamel disappears, the symptoms will become more pronounced.
This pathology requires immediate consultation with a doctor while the symptoms indicate initial stage diseases. If left untreated, the consequences of the disease can be deformation of the joints, changes in the lower part of the face, and the appearance of severe pain.
Diagnosis of the disease
Diagnosis of pathological abrasion of tooth enamel includes an in-depth analysis of symptoms. Because of wide range Symptoms of abrasion can only be diagnosed by a dentist, taking into account all factors and the possible presence of other pathologies.
The examination scheme includes:

- A complete examination and interview of the patient, studying the history of the disease to determine the forms and stage of the pathology.
- Inspection of external signs.
- Complete examination of the oral cavity and the condition of the patient’s masticatory muscles.
- Study of the functions of the temporal and mandibular joints.
To study the picture of the disease, radiography, tomography, and electromyography can be used.
The initial examination of the patient's face includes studying the contours of the face, its symmetry and proportionality. Specialists analyze the degree of destruction of the mucous membrane, the level of tooth wear, and the condition of hard tissues to determine possible complications during treatment.
Examination of the masticatory muscles allows one to study their condition, possible asymmetry and hypertonicity. In this case, electromyography is often used. All this helps to minimize possible complications.

Examination of the temporal and mandibular joints allows us to determine different kinds pathologies that can occur with this type of disease.
Electroodontodiagnosis, or EDI. This type of diagnosis is necessary, since in the pathology of tooth abrasion, the death of the pulp very often occurs, while the patient did not observe any signs of deviation. EDI is prescribed only for the second or third stages of the disease, since in the initial stage symptoms do not appear.
Diagnostics allows us to identify the main causes of increased tooth abrasion. In addition to the oral cavity, doctors focus on the condition of the temporal and mandibular joints.
Forms of treatment
Treatment of this problem takes a lot of time, this is due to a huge variety of factors influencing the problem. In addition, it is important to determine the stage of development of the disease, this will help choose the right treatment and speed up the process.

To cure pathological abrasion of the first and second degrees, doctors first stabilize the already advanced process so that the disease does not develop.
At the initial stage, doctors install temporary prostheses (to begin the recovery process and maintain chewing functions). After positive dynamics are observed, temporary prostheses are replaced with permanent ones.
Treatment more advanced stages diseases (third and fourth) begins with restoration of the bite. At this stage, experts strictly prohibit the installation of crowns, as this may cause the appearance of malocclusion at the patient. As a result of their establishment, tooth tissue may be damaged.
Making prosthetics is an important issue. At the initial levels of development of this disease, prostheses are most often made from plastic, ceramics, and sometimes the choice falls on prostheses made from precious metals. In cases where the disease has progressed, prostheses made of ceramic or metal ceramics are often used.
When installing prostheses, it is important to remember that the prostheses must be made of the same materials, otherwise You can come to the opposite (repeated) bite correction.
If the cause of pathological tooth wear is heavy load or periodic contraction of the masticatory muscles, experts recommend installing dentures that are not susceptible to cracks (more durable): made of metal-plastic or metal. In this case, metal ceramics are strictly prohibited.
Main stages of treatment:
- By installing temporary dentures, doctors correct the height of the bite.
- The adaptation of teeth to the new position is analyzed.
- After positive results, temporary dentures are replaced with permanent ones.
Restoring the height of the bite at the first stage occurs through the installation of so-called plastic aligners.

The adaptation period is the patient's adaptation to other jaw positions. Most often, this period is characterized by severe discomfort. The patient must attend dental office at least twice a week, this is necessary for strict control and research of the results of wearing aligners by the dentist. More often average duration Wearing temporary aligners takes about two to three weeks. It is also necessary to take into account that adaptation begins from the moment the patient stops complaining of discomfort in the temple area, mandibular joint, as well as in the area of the masticatory muscles when eating food.
The third stage of treatment is the installation of permanent prostheses (final prosthetics). At this stage, special materials are selected to achieve the preservation of a correctly established bite. To achieve the best possible results, when making prostheses, doctors take into account the results obtained when wearing therapeutic mouth guards, which were installed temporarily.

The process of permanent prosthetics can take place either immediately or in stages. Aligners help determine the exact occlusal height for the patient. For the remaining areas, prostheses begin to be made after complete fixation of the first permanent prostheses.
Prevention of tooth wear
To protect yourself from the disease or from its reoccurrence, you must adhere to the following rules and recommendations:

Treatment prognosis
The prognosis for treatment of this disease is generally positive. Of course, treatment takes a much shorter period of time if the patient applies in the early stages of the disease. In addition, younger patients are more likely to recover quickly. However, relapses of pathological tooth wear often occur, so dentists talk about the need to register patients suffering from this pathology.

Pathological abrasion of teeth- pathological condition of the dental system of polyetiological origin. Characterized by excessive loss of enamel or enamel and dentin of all or only individual teeth.
Pathological abrasion of teeth occurs in middle-aged people, reaching the highest frequency (35%) in 40-50-year-olds, and is more common in men than in women. Against the background of congenital developmental pathology, pathological abrasion of teeth is observed in people and adolescents.
Etiology and pathogenesis
The occurrence of pathological tooth abrasion is associated with the action of various etiological factors, as well as their various combinations.
Conventionally, we can distinguish 3 groups of causes of pathological tooth abrasion:
1) functional deficiency of hard dental tissues;
2) excessive abrasive effect on hard tissues teeth;
3) functional overload of teeth.
Functional deficiency of hard dental tissues. This deficiency may be a consequence of endogenous and exogenous factors. Endogenous factors include congenital or acquired pathological processes in the human body that disrupt the process of formation, mineralization and vital activity of dental tissue.
Congenital functional deficiency of hard tissues of teeth can be a consequence of pathological changes in ectodermal cell formations (enamel deficiency) or pathological changes in mesodermal cell formations (dentin deficiency) or a combination of both. At the same time, such a developmental disorder can be observed in some general somatic hereditary diseases: marble disease (congenital diffuse osteosclerosis or osteoporosis of almost the entire skeleton); Porac-Durant syndrome, Frolik syndrome (congenital osteogenesis imperfecta) and Lobstein syndrome (late osteogenesis imperfecta). This group of hereditary lesions includes Capdepont dysplasia.
With marble disease, slow development of teeth, their late eruption and changes in structure with pronounced functional deficiency of hard tissues are noted. The roots of the teeth are underdeveloped, the root canals are usually obliterated. Odontogenic inflammatory processes are characterized by severity and often develop into osteomyelitis.
In Frolik and Lobstein syndromes, the teeth are of normal size and correct form. The color of the crowns of the teeth is characteristic - from gray to brown with a high degree of transparency. The degree of staining of different teeth in the same patient is different. Wear is more pronounced in incisors and first molars. Dentin of teeth in this pathology is not sufficiently mineralized, the enamel-dentin junction looks like a straight line, which indicates its insufficient strength.
The same picture can be observed with Capdepont syndrome. Teeth of normal size and shape, but with altered coloring, different for different teeth of the same patient. Most often the color is watery-gray, sometimes with a pearlescent sheen. Soon after teeth erupt, the enamel chips off, and the exposed dentin, due to its low hardness, quickly wears out. Impaired mineralization of dentin leads to a decrease in its microhardness by almost 1.5 times compared to the norm. The tooth cavity and root canals are obliterated. The electrical excitability of the pulp of worn teeth is sharply reduced. Affected teeth react poorly to chemical, mechanical and temperature stimuli.
Obliteration of the tooth cavity and root canals with this dysplasia begins during the process of tooth formation, and is not a compensatory reaction to pathological abrasion. In the area of the root tips, rarefaction is often noted bone tissue.
In contrast to functional dental deficiency in Frolik and Lobstein syndromes, Capdepont dysplasia is inherited as a permanent dominant trait.
Acquired etiological endogenous factors of pathological tooth abrasion include a large group of endocrinopathies in which mineral, mainly phosphorus-calcium, and protein metabolism are disrupted.
Hypofunction of the pituitary gland of the anterior lobe, accompanied by a deficiency of somatotropic hormone, inhibits the formation of the protein matrix in the elements of the mesenchyme (dentin, pulp). A deficiency of pituitary gonadotropic hormone has the same effect.
Violation of the secretion of adrenocorticotropic hormone from the pituitary gland leads to activation of protein catabolism and demineralization.
Pathological changes in the hard tissues of teeth in cases of dysfunction of the thyroid gland are associated mainly with hyposecretion of thyrocalcitonin. In this case, the transition of calcium from the blood to the tooth tissue is disrupted, i.e., the plastic mineralizing function of the dental pulp changes.
The most pronounced disturbances in the hard tissues of teeth are observed when the function of the parathyroid glands changes. Parathyroid hormone stimulates osteoclasts, which contain proteolytic enzymes (acid phosphatase), which contribute to the destruction of the protein matrix of hard dental tissues. At the same time, calcium and phosphorus are excreted in the form of soluble salts - citrate and lactic acid calcium. Due to a deficiency in the activity of the enzymes lactate dehydrogenase and isocitrate dehydrogenase in osteoblasts, carbohydrate metabolism is delayed at the stage of formation of lactic and citric acids. As a result, highly soluble calcium salts are formed, the leaching of which leads to a significant decrease in the functional value of hard dental tissues.
Another mechanism of demineralization of hard dental tissues in pathology of the parathyroid glands is hormonal inhibition of phosphorus reabsorption in the kidney tubules.
Dysfunctions of the adrenal cortex and gonads also lead to demineralization of hard dental tissues and increased protein catabolism.
Neurodystrophic disorders are of particular importance in the occurrence of functional deficiency of hard dental tissues, leading to pathological abrasion. Irritation of various parts of the central nervous system (CNS) in the experiment led to increased abrasion of enamel and dentin of teeth in experimental animals.
Exogenous factors of functional deficiency of hard dental tissues include, first of all, nutritional deficiency. Malnutrition (lack of minerals, protein deficiency of foods, unbalanced diet) disrupts metabolic processes in the human body and, in particular, the mineralization of hard dental tissues.
Functional deficiency of hard dental tissues due to insufficient mineralization can result from delayed absorption of calcium in the intestine due to vitamin D deficiency, deficiency or excess of fat in food, colitis, and profuse diarrhea. These factors become most important during the formation and eruption of teeth. The lack of vitamins D and E in the patient’s body, as well as hypersecretion of parathyroid hormone, inhibit the reabsorption of phosphorus in the renal tubules and contribute to its excessive excretion from the body, disrupting the process of mineralization of hard tissues. Such demineralization is also observed in kidney diseases.
Chemical damage to hard dental tissues occurs in chemical production and is an occupational disease. Acid necrosis of hard dental tissues is also observed in patients with achilic gastritis who take hydrochloric acid orally. It is necessary to emphasize the great sensitivity of tooth enamel to acid exposure.
Already in the initial stages of acid necrosis, patients develop a feeling of numbness and soreness in their teeth. Pain may occur when exposed to temperature and chemical stimuli, as well as spontaneous pain. Sometimes patients complain of a feeling of teeth sticking when they are closed.
As replacement dentin is deposited and dystrophic and necrotic changes occur in the pulp of the affected teeth, these sensations become dull or disappear. Typically, acid necrosis affects the front teeth. The enamel disappears in the area of the cutting edges, and the underlying dentin is involved in the process of destruction. Gradually, the crowns of the affected teeth, being worn and destroyed, shorten and become wedge-shaped.
Significant violation functional state hard tissues of teeth is found in conditions of phosphorus production. Necrotic changes in the structure of dentin were noted, in some cases - the absence of replacement dentin, an unusual structure of cement, similar to the structure of bone tissue.
Among physical factors, reducing the functional value of hard dental tissues and leading to the development of pathological abrasion of teeth, radiation necrosis occupies a special place. This is explained by an increase in the number of patients subjected to radiation therapy in the complex treatment of oncological diseases of the head and neck region. In this case, radiation damage to the pulp is considered primary, which manifests itself in microcirculation disturbances with symptoms of pronounced plethora in the precapillaries, capillaries and venules, perivascular hemorrhages in the subodontoblastic layer. In odontoblasts, vacuolar degeneration and necrosis of individual odontoblasts are observed. In addition to diffuse sclerosis and petrification, the formation of denticles of different sizes and locations is observed, varying degrees organization. In all areas of dentin and cement, demineralization phenomena and areas of destruction are detected. These changes in hard tissues occur at different times after irradiation and depend on the total dose. The greatest changes in dental tissues are observed in the period from the 12th to the 24th month after radiation therapy for tumors in the head and neck area. As a result of significant destructive lesions of the pulp, changes in hard tissues are irreversible.
For the prevention of dental damage during radiation therapy of diseases maxillofacial area It is necessary to cover the teeth during the irradiation session with a plastic mouthguard such as a boxing splint, carry out thorough sanitation, and proper hygienic care.
The second group of etiological factors for pathological tooth abrasion consists of factors of different nature, the common point of which is an excessively abrasive effect on the hard tissues of the teeth. Resident survey data Yamalo-Nenets District[Lyubomirova I.M., 1961] revealed a large number of severe cases of pathological abrasion of teeth down to the gum level as a result of residents eating very hard food - frozen meat and fish.
S. M. Remizov's long-term observations of the abrasive effect of toothbrushes, tooth powder and toothpastes of various designs convincingly showed that incorrect, irrational use of hygiene and dental care products can turn from a therapeutic and prophylactic agent into a formidable destructive factor leading to pathological abrasion of teeth. Normally, there is a significant difference in the microhardness of enamel (390 kgf/mm2) and dentin (80 kgf/mm2). Therefore, the loss of the enamel layer leads to irreversible wear of the teeth due to the significantly lower hardness of dentin.
Industrial dust in highly dusty enterprises (mining industry, foundry) also has a strong abrasive effect on the hard tissues of teeth. Significant pathological abrasion of teeth occurs among coal mine workers.
IN Lately in connection with the widespread introduction into orthopedic dental practice prostheses made of porcelain and metal-ceramics, cases of pathological abrasion of teeth have become more frequent, the cause of which is the excessive abrasive effect of a poorly glazed surface of porcelain and ceramics.
The study of the surface of natural teeth and dentures made of various ceramic materials made it possible to establish that the surface of a natural tooth is smooth, without roughness or protrusions, and visible scratches are a consequence of mechanical wear. The condition of the porcelain surface has a sharp difference, which consists in the presence of a significant number of irregularities of a pointed, point-like shape or in the form of vitrified areas with the inclusion of sharp grains. Samples made from Sikor have a more uniform surface. Visible roughnesses are smaller in size with a large radius of curvature. However, disruption of the glossy surface reveals the porous nature of the base material. The cast glass sample has a smooth surface, free of protrusions and roughness.
As a rule, the state of the surface is characterized by the number of irregularities per unit area and the radius of curvature of the tops of these irregularities. When interacting between antagonistic teeth, the main importance is the actual contact area, which is directly proportional to the magnitude of the load and inversely proportional to the microhardness of the material. Knowing the condition of the surface of the material (the density of irregularities and the radius of their curvature), it is possible to approximately estimate the area of their contact and the maximum loads at which the destruction of the surface begins. Comparison of the surface condition of porcelain and glass-ceramic prostheses obtained different ways, gives grounds to assert that the size and density of surface roughness of dental crowns is determined by the method of their manufacture. The formation of the surface of porcelain dentures occurs during the sintering process of multicomponent powders, including components of different refractoriness. Sharp protrusions are the most refractory components of the material; these areas, due to increased refractoriness, and therefore high viscosity(during the sintering process) cannot be leveled by surface tension forces.
The basis for the manufacture of sycor products is homogeneous glass melt, which eliminates the appearance of significant inhomogeneities on their surface. However, the powder sintering method involves uneven surface tension during the sintering process, which results in the presence of individual protrusions on the surface. Mechanical polishing does not smooth out roughness due to the fact that the glaze film is opened and the roughness increases.
Thus, glass-ceramic dentures, especially those made by casting (V.N. Kopeikin, I.Yu. Lebedenko, S.V. Anisimova, Yu.F. Titov), compared with porcelain dentures produced by powder sintering, have a much smoother surface that does not change during long-term use due to the fine-crystalline structure of glass ceramics and the absence of pores in it. Violation of the glazed layer of dentures, which occurs during grinding of glass-ceramic and porcelain dentures fixed in the mouth, sharply increases the surface roughness and, consequently, the coefficient of its friction with the antagonist, which, together with the high hardness of the material, can lead to intense abrasive wear of the hard tissues of the antagonist teeth . Therefore, when making dentures from ceramic materials, in order to prevent complications in the form of pathological abrasion of opposing teeth, it is necessary to carefully check the occlusal contacts at the stage of fitting the dentures, and be sure to glaze the surface of the ceramic dentures well without disturbing it after fixation.
Pathological abrasion of teeth may be a consequence of the nature of chewing, in which all teeth or only part of the teeth experience excessive functional load.
In such cases, excessive functional load over time can lead to two types of complications: from supporting apparatus teeth - periodontal or from the side of the hard tissues of the teeth - pathological abrasion of teeth, which more often occurs against the background of functional deficiency of hard tissues, although it can also be observed in teeth with normal structure and mineralization of enamel and dentin. Overload of teeth can be focal or generalized.
One of the reasons for focal functional overload of teeth is bite pathology. In the presence of pathology in the process of chewing in various phases of occlusion, certain groups of teeth experience excessive load and, as a result, pathological abrasion of teeth occurs. An example is the abrasion of the palatal surface of the anterior teeth of the upper row and the vestibular surface of the lower jaw incisors in patients with a deep blocking bite. Common cause Pathological abrasion of individual teeth is an anomaly in the position or shape of a tooth, leading to the occurrence of supercontact on this tooth during function.
The type of bite can also aggravate the development of pathological abrasion of teeth, resulting from functional inferiority of hard tissues of teeth or excessive abrasive effects of various factors. Thus, with a straight bite, the processes of erasing hard tissues proceed much faster than with other types of bite.
Partial adentia (primary or secondary), especially in the area of chewing teeth, leads to functional overload of the remaining teeth. With bilateral loss of chewing teeth, the front teeth experience not only excessive, but also unusual functional load. In this case, pathological abrasion of the remaining antagonizing teeth is observed.
Medical errors in the prosthetic treatment of dentition defects also lead to excessive functional load: the lack of multiple contacts of teeth in all phases of all types of occlusion causes overload of a number of teeth and their wear. Often there is abrasion of individual teeth that antagonize teeth that have protruding fillings made of composite materials, due to the inherent strong abrasive effect of composites.
In orthopedic dentistry there is currently a large arsenal of materials for the manufacture of dentures. When using them, you should strictly follow the indications and pay attention to Special attention on the possibility of their combined use.
For example, plastic for fixed dentures “Sinma” is inferior in hardness to tooth enamel. Therefore, when making plastic prostheses (bridges with an open chewing surface or removable dentures) in the area of chewing teeth, it is inevitable that functional overload of the anterior teeth due to wearable plastic will inevitably occur in the immediate period after prosthetics. Another example: in the combined production of dentures from precious metals and plastic antagonists, plastic, due to its inherent high abrasive effect, will lead to rapid wear of crowns made of precious alloys, and consequently to a functional overload of the antagonistic natural teeth present in the mouth. When assessing abrasive wear, one should take into account not only the hardness of the material, but also the magnitude of its coefficient of friction with the antagonist material: the higher the coefficient of friction, the more significant the abrasive effect of the material. For example, the hardness of Sikor sital is higher than the hardness of Vitadur porcelain, but its abrasive effect is less, since its coefficient of friction with the tissues of natural teeth is lower.
One of the causes of generalized pathological wear of teeth is considered to be bruxomania, or bruxism - unconscious (usually at night) clenching of the jaws or habitual automatic movements of the lower jaw, accompanied by grinding of teeth. Bruxism occurs in both children and adults. The causes of bruxism are not well understood. It is believed that bruxism is a manifestation neurotic syndrome, is also observed with excessive nervous tension. Bruxism belongs to parafunctions, i.e. to a group of perverted functions.
The role of functional overload of teeth in the etiology of pathological tooth abrasion was proven in an experiment on animals [Kalamkarov Kh. A., 1984]. The overload of the anterior teeth was simulated by removing chewing teeth or making crowns for the anterior teeth of the lower jaw to increase the bite.
As a result, after only 3 months, significant wear of the cutting edge of the anterior teeth was noted. At histological examination It has been established that morphological changes during pathological abrasion of teeth due to functional overload take place in all periodontal tissues.
With pathological abrasion of teeth, in most cases, in response to the loss of hard tissues, replacement dentin is formed according to the localization of the abraded surface. The amount of replacement dentin varies and is not related to the degree of wear. With massive deposition of replacement dentin, its globular structure is noted. The tooth cavity decreases in volume until complete obliteration.
The configuration of the altered dental cavity depends on the topography of the abrasion and the degree of damage. The formation of denticles of various shapes, sizes and degrees of maturity is often observed.
There are significant changes in the pulp of pathologically worn teeth (Fig. 85). They are expressed, in particular, as follows:
In changes in vascularization: depletion of the pulp with blood vessels, sclerosis of blood vessels; sometimes, on the contrary, increased vascularization and small foci of hemorrhage are observed; in partial or complete vacuolization, atrophy of odontoblasts, a decrease in the number of cellular elements; in reticular atrophy, sclerosis, pulp hyalinosis.
Rice. 85. Vacuolation of the odontoplast layer with pathological abrasion. Microphoto.
The severity of pulp damage depends on the degree of pathological abrasion of teeth. In the nervous apparatus of the pulp, changes in the type of irritation are noted: hyperargyrophilia, thickening of the axial cylinders.
Typical for pathological abrasion of teeth with functional overload (more than 80%) is a compensatory increase in the thickness of the cement tissue - hypercementosis (Fig. 86).
In this case, the layering of cement occurs unevenly, the greatest is observed at the root apex. Not only does the mass of cement increase, but often its structure takes on a layered appearance.
Cementicles are often found. In some patients, destruction of cement with its partial peeling from dentin is observed, which can be regarded as osteoclastic resorption of root tissue in response to functional overload.
Changes in the periodontium with pathological abrasion of teeth due to functional overload consist in the unevenness of the width of the periodontal gap along the gingival margin to the root apex. The expansion of the periodontal fissure occurs more in the cervical part and at the apex of the root and directly depends on the degree of functional overload.

Rice. 86. Hypercementosis of the tooth due to abrasion. Microphoto.
In the middle third of the root, the periodontal fissure is usually narrowed. In all cases, local hemodynamic disturbances, edema, hyperemia, and focal infiltration are noted. Often, in response to excessive functional load, the periodontium of worn teeth develops chronic inflammation with the formation of granulomas and cystogranulomas, which must be taken into account when examining such patients and choosing a treatment plan (Fig. 87).
Pathological abrasion of teeth leads to a change in the shape of the crown part, which in turn contributes to a change in the direction of action of the functional load on the tooth and periodontium. At the same time, zones of compression and tension arise in the latter, which necessarily leads to characteristic pathological changes in the periodontium. In areas of compression, cement resorption, its peeling from dentin, replacement with osteocement, osteoclastic resorption of bone tissue, and periodontal collagenization are noted. In tension zones, on the contrary, there is a massive layering of cement, along the periphery of which there is deposition of osteocement.

Rice. 87. Resorption of the apex of the tooth root. A granuloma is also visible. Microphoto.
Changing the shape of the coronal part with pathological tooth wear (PAW) increases the functional load on the teeth.
Thus, with pathological abrasion of teeth resulting from functional overload, a vicious circle is observed: functional overload leads to pathological abrasion of teeth, a change in the shape of the crowns, which in turn changes the functional load necessary for chewing food, increasing it, and this is even more promotes the destruction of hard tissues of teeth and periodontium, exacerbating pathological abrasion. Therefore, orthopedic treatment aimed at restoring the normal shape of worn teeth should be considered not symptomatic, but pathogenetic.
Clinical picture
The clinical picture of pathological tooth abrasion is extremely diverse and depends on the degree of damage, topography, prevalence and duration of the process, its etiology, the presence of concomitant general pathology and lesions of the dentofacial system.
With pathological abrasion of teeth, aesthetic standards are first violated due to changes in the anatomical shape of the teeth. Subsequently, with the progression of the pathological process and significant shortening of the teeth, chewing and phonetic functions change. In addition, some patients, even in the initial stages of pathological tooth wear, experience hyperesthesia of the affected teeth, which interferes with the intake of hot, cold, sweet or sour foods.
To classify the entire diversity clinical manifestation pathological abrasion of teeth is distinguished by forms, types and degree of damage. The forms of pathological tooth abrasion characterize the extent of the pathological process. There are generalized and localized forms.
A generalized form of pathological tooth wear, in turn, can be accompanied by a decrease in occlusal height (Fig. 88).
Types of pathological abrasion of teeth reflect the predominant plane of tooth damage: vertical, horizontal or mixed damage (Fig. 89).
The degree of pathological abrasion of teeth characterizes the depth of the lesion: I degree - damage to no more than 1/3 of the height of the crown; II degree - damage to 1/3 - 2/3 of the crown height; III degree - damage to more than 2/3 of the tooth crown.
The pathological process can affect the teeth of one or both jaws, on one or both sides. In practice, there are cases of varying degrees of damage to the teeth of one or both jaws. The nature and plane of the lesion may be identical, but may also differ. All this determines the diversity of the clinical picture of pathological tooth wear, which becomes significantly more complicated when one or both jaws are partially edentulous.

Rice. 88. Abrasion: generalized form.
To make a correct diagnosis and choose the optimal treatment plan for such a diverse clinical picture of pathological tooth abrasion, it is necessary to carefully examine patients to identify the etiological factors of pathological tooth abrasion and concomitant pathology. The examination must be carried out in full according to the traditional scheme: 1) interviewing the patient, studying complaints, life history and medical history; 2) external inspection; 3) examination of the oral cavity; palpation of the masticatory muscles, temporomandibular joint, etc.; 4) auscultation of the temporomandibular joint; 5) auxiliary methods: study of diagnostic models, targeted radiography of teeth, panoramic radiography of teeth and jaws, EDI, tomography, electromyography and electromyotonometry of masticatory muscles.
Complaints of patients can be different and depend on the degree of pathological abrasion of teeth, topography and extent of the lesion, duration of the disease, and concomitant pathology.
In the absence of concomitant lesions of the maxillofacial area, patients with pathological abrasion of teeth usually complain of a cosmetic defect due to the progressive loss of hard dental tissues, sometimes hyperesthesia of enamel and dentin, and with acid necrosis - a feeling of soreness and roughness of the enamel.

Rice. 89. Types of pathological abrasion.
a - vertical; 6 - horizontal.
When studying the patient’s life history, pay attention to the presence similar pathology in other family members, which may indicate genetic predisposition, congenital functional deficiency of hard dental tissues.
It should be borne in mind that pathological abrasion of teeth can be observed in several members of the same family and not only as a result of hereditary pathology, but also due to common diet, everyday life, and sometimes occupational hazards. All this can contribute to a decrease in the functional value of hard dental tissues and increased abrasive wear.
When collecting anamnesis, it is necessary to identify concomitant general somatic pathology, congenital dysplasia, endocrinopathies, neurodystrophic disorders, kidney diseases, gastrointestinal tract etc. It is necessary to very carefully identify the root cause of abrasion. If from the anamnesis and as a result of a clinical examination it turns out that pathological abrasion of teeth arose against the background of a functional deficiency of hard dental tissues of endogenous origin, then when choosing a prosthesis design, one should prefer those that would minimally overload the supporting teeth. Otherwise, due to congenital (especially) or acquired deficiency in osteogenesis, resorption of the roots and severe atrophy of bone tissue from the dental alveoli may occur.
Often, with hereditary diseases (marble disease, Frolik's syndrome, etc.), the roots of worn teeth are underdeveloped, the root canals are curved and obliterated. Therefore, in such cases, the indications for pin structures are narrowed. In addition, clarifying the history of hereditary pathology such as Frolik and Lobstein syndromes, Capdepont syndrome makes it possible to predict with a sufficient degree of probability the prognosis of the state of the dental system and the musculoskeletal system as a whole in subsequent generations, since dental changes in Frolik and Lobstein syndromes are inherited as an unstable dominant sign, and in Capdepont syndrome - as a permanent dominant sign.
When clarifying the history of the present disease, attention is paid to the age of occurrence of pathological tooth abrasion, the nature of its progression, the connection with prosthetics of teeth and jaws, the nature and working conditions and living conditions of the patient.
During an external examination of the patient’s face, the facial configuration, proportionality and symmetry are noted. Determine height lower section faces in a state of physiological rest and in central occlusion. The condition of the hard tissues of the teeth is carefully studied, establishing the nature, extent, and degree of wear. Pay due attention to the condition of the oral mucosa and periodontal teeth to identify concomitant pathologies and complications.
Palpation of the masticatory muscles reveals pain, asymmetry of sensations, swelling of the muscles, their hypertonicity and suggests the presence of parafunctions in the patient. In the future, to clarify the diagnosis, it is necessary to carry out additional research: electromyography and electromyotonometry of the masticatory muscles, consult with a neurologist about possible bruxism, carefully question the patient and his relatives about possible grinding of teeth in sleep. This is necessary to prevent complications and select the optimal comprehensive treatment for such a contingent of patients.
Palpation of the temporomandibular joint area, as well as auscultation of this area, allows us to identify pathology, which is often found in pathologically worn teeth, especially in the generalized or localized form, complicated by partial edentia. In these cases, careful analysis of diagnostic models and x-ray examination are necessary; frontal and lateral tomograms with closed jaws and physiological rest.
Electroodontodiagnosis (EDD) is mandatory diagnostic test with pathological abrasion of teeth, especially II and III degrees, as well as when choosing the design of fixed dentures. Often, pathological abrasion of teeth is accompanied by asymptomatic death of the pulp.
As a result of the deposition of replacement dentin, partial or complete obliteration of the pulp chamber, the electrical excitability of the pulp is reduced. In case of pathological abrasion of teeth of the first degree, accompanied by hyperesthesia of hard tissues, EDI usually does not reveal deviations from the norm.
Just like EDI, radiography (sighted and panoramic) is a mandatory diagnostic method that allows us to establish the size and topography of the pulp chamber, topography, direction and degree of obliteration of the root canals, the severity of hypercementosis, the presence of cysts, which are often found with functional overload of teeth, and granulomas in worn teeth. All this without a doubt has great importance to choose the right treatment plan.
Correct diagnosis and treatment planning for patients with pathological tooth wear, as well as monitoring the progress and results of treatment, is facilitated by a thorough study of diagnostic models. Using diagnostic models, the type, shape and degree of pathological abrasion of teeth, the condition of the dentition are specified, and when analyzed in an articulator, the nature of the occlusal relationships of teeth and dentition in various phases of all types of occlusion, which is especially important when diagnosing concomitant pathology of the temporomandibular joint and choosing a treatment plan.
Treatment
Restoring the anatomical shape of worn teeth depends on the degree, type and shape of the lesion. To restore the anatomical shape of teeth in case of pathological wear of teeth of the first degree, inlays, fillings (mainly on the front teeth), and artificial crowns can be used; II degree - inlays, artificial crowns, clasp dentures with occlusal overlays; III degree - stump crowns, stamped caps with occlusal soldering.
In case of pathological abrasion of teeth of II and III degrees, conventional stamped crowns cannot be used, since complications associated with trauma to the marginal periodontium by the edge of the crown, deeply advanced into the gingival pocket, are possible. Deep advancement of a stamped crown can occur when the crown is cemented onto a severely shortened tooth. In addition, trauma to the marginal periodontium is also possible during the use of a crown, when, under the action of chewing pressure, a thick layer of cement between the chewing surface of the worn tooth and the occlusal surface of the crown is destroyed and the crown is deeply immersed in the gingival pocket. Therefore, if there are indications for the treatment of pathological wear of teeth with artificial crowns, several options for their manufacture are possible (Fig. 90, 91): 1) solid crowns; 2) stamped caps with occlusal soldering; 3) stump crowns (stamped or cast crowns) with preliminary restoration of the height of the tooth crown with a stump inlay with a pin.
When choosing a material for crowns, you should consider its wear resistance. If the antagonist teeth have unaffected enamel, metal, metal-ceramic, or porcelain crowns can be used. For antagonists with I degree of pathological abrasion, plastic crowns, metal crowns made of stainless steel, alloys of precious metals are preferred; ceramic and solid-cast prostheses from KHS.

Rice. 90. Crowns for the treatment of pathological abrasion, a - frame of a fenestrated metal crown; b - stamped cap with holes on the chewing surface; c, d — plastic is applied to the crown and cap; d — solid-cast frame of a metal-plastic crown.

Rice. 91. Fixed dentures such as pins and caps with an occlusal cast part to restore the shape of teeth in case of pathological abrasion.
Counter prosthetics with inlays and (or) crowns using structural materials of equal wear resistance are indicated for antagonists with II - III degrees of pathological abrasion.
In case of pathological abrasion of teeth resulting from bruxism and parafunctions, preference should be given to solid metal and metal-plastic (with a metal chewing surface) dentures made of base metal alloys as they are more resistant to abrasion. Metal-ceramic dentures in such patients should be used limitedly due to the possible chipping of the coating due to involuntary non-functional excessive occlusal overload: night grinding of teeth, spastic clenching of the jaws, etc.
When choosing a treatment plan for pathological tooth wear complicated by partial edentia (Fig. 92), be sure to base it on data from EDI and X-ray monitoring of supporting teeth. When pathological abrasion of teeth occurs against the background of congenital disorders of amelo- and dentinogenesis, imperfections of the roots of the teeth, their functional disability, which can lead to resorption of the roots of such teeth when used as supports for bridges. Such patients are recommended to restore worn teeth with artificial crowns or inlays, followed by the manufacture of removable (clasp or plate) dentures (Fig. 93).
Treatment of pathological tooth wear complicated by a decrease in occlusal height. Treatment is carried out in several stages: 1) restoration of occlusal height with temporary therapeutic and diagnostic devices; 2) adaptation period; 3) permanent prosthetics.
At the first stage, the occlusal height is restored using plastic dental aligners, dentogingival aligners, removable plate or clasp dentures with overlapping of the chewing surface of worn teeth. Such restoration can be immediate when the occlusal height is reduced to 10 mm from the height of physiological rest, and gradual - 5 mm every 1-12 months when the occlusal height is reduced by more than 10 mm from physiological rest (Fig. 94).
To establish the height of the future prosthesis, wax or plastic bases with bite ridges are made, determined and fixed in a generally accepted way In the clinic, the required “new” position of the lower jaw is required; X-ray control is required. On radiographs of the temporomandibular joints with closed dentition in a position fixed with wax rollers, there should be a “correct” position of the articular head (on the slope of the articular tubercle) uniform on both sides. Only after this is this position fixed with temporary therapeutic and diagnostic prosthetic devices.
The second stage - an adaptation period lasting at least 3 weeks - is required for the patient to completely get used to the “new” occlusal height, which occurs due to the restructuring of the myotatic reflex in the masticatory muscles and the temporomandibular joint.

Rice. 92. Bridge prosthesis used for pathological abrasion.
a - soldered prosthesis frame; b - the frame is lined with plastic; c - solid cast prosthesis frame (left) and frame lined with pyroplast (right).

During this period, the patient should be under the dynamic supervision of the attending orthopedic dentist (at least once a week, and if necessary: subjective discomfort, pain, discomfort, inconvenience when using diagnostic and treatment devices - and more often).
When using non-removable therapeutic and diagnostic devices - plastic mouth guards - the adaptation process proceeds faster than when restoring the occlusal height with removable structures, especially plate ones. This is explained not only by the design features of the prostheses, but also by the fact that non-removable mouth guards are fixed with cement and patients use them constantly. On the contrary, patients often use removable devices only for a short time of the day, removing them while working, eating, or sleeping. Such use of prosthetic devices should be regarded not only as useless, but as harmful, since it can lead to pathological changes in the temporomandibular joint and muscle-articular dysfunction.
Therefore, it is necessary to conduct preliminary explanatory conversations with patients with a warning about possible complications due to inconsistent use of the medical device and the need for mandatory contact with the attending orthopedic dentist if unpleasant sensations occur in the temporomandibular joint, masticatory muscles, or the mucous membrane of the prosthetic bed. At the time of fitting the diagnostic and treatment apparatus and during control examinations, occlusal contacts are especially carefully checked in all phases of all types of occlusion, the quality of polishing of the prosthesis is checked, the absence of sharp protrusions and edges that can injure soft tissues.
If, with a simultaneous increase in the occlusal height by 8-10 mm, the patient experiences severe pain that increases during the first week in the area of the temporomandibular joint and (or) masticatory muscles, it is necessary to reduce the height by 2-3 mm until the pain disappears, and then , after 2-3 weeks, re-increase the occlusal height to the required value. Technically, this can be easily done by grinding off the layer of plastic on the chewing surface of the diagnostic and treatment device or applying an additional layer of quick-hardening plastic.
It must be emphasized that the adaptation period of 2-3 weeks is considered from the moment the patient’s last unpleasant sensations in the area of the temporomandibular joint or masticatory muscles disappear.
Sometimes, due to unpleasant subjective sensations, repeated attempts to increase the occlusal height to the desired optimal level (2 mm below the height of physiological rest) remain unsuccessful. For such patients, permanent dentures are made at the maximum occlusal height to which he was able to adapt. This is usually observed in patients in whom a decrease in occlusal height occurred more than 10 years ago and irreversible changes have occurred in the temporomandibular joint. The same picture is observed in patients with pathological abrasion of teeth, complicated by disorders of the psycho-emotional sphere, who overly focus on the nature and degree of their subjective sensations. Orthopedic treatment of pathological tooth wear, complicated by a decrease in occlusal height, in this category of patients is extremely difficult, the prognosis is questionable, and treatment must be carried out in parallel with treatment by a neuropsychiatrist.
The third stage of treatment - permanent prosthetics - is not fundamentally different in the type of denture designs used in the treatment of pathological tooth wear. It is only important to note the need to use structural materials that guarantee the stability of the established occlusal height. The use of plastic on the chewing surface of bridges is unacceptable. In removable dentures, it is preferable to use porcelain teeth and cast occlusal overlays (Fig. 95). To stabilize the occlusal height, counter inlays and crowns are used.
An important condition for achieving good results in permanent prosthetics is the manufacture of prostheses under the control of temporary therapeutic and diagnostic aligners. It is possible to manufacture permanent dentures in stages. First, dentures are made for one half of the upper and lower jaws in the area of the chewing teeth, while temporary aligners remain fixed in the frontal area and on the opposite half of both jaws.

Rice. 95. Pathological abrasion; mixed form(s). Clasp denture with occlusal overlay in the group of chewing teeth (b) and metal-ceramic crowns on the front group of teeth (c).
When fitting permanent dentures, temporary aligners allow you to accurately establish the occlusal height and optimal occlusal contacts in various phases of all types of occlusion to which the patient is adapted. After fixing the permanent dentures on one half of the jaws, the temporary aligners are removed and the production of permanent dentures for the rest of the dentition begins. During the production of prostheses, therapeutic and diagnostic mouthguards are temporarily fixed.
Treatment of pathological tooth wear without reducing occlusal height. Treatment is also carried out in stages. At the first stage, using the method of gradual disocclusion, the area of the dentition with pathological wear of teeth and vacant hypertrophy of the alveolar process is reconstructed, achieving sufficient occlusal space to restore the anatomical shape of worn teeth (Fig. 96). To do this, a plastic mouth guard is made on the teeth that are in opposition to the teeth to be “rebuilt.” Comply next rule: the sum of the periodontal endurance coefficients of the teeth included in the mouthguard should be 1.2-1.5 times higher than the sum of the periodontal endurance coefficients of the teeth subject to “restructuring”.

Rice. 96. Therapeutic mouth guard made of plastic for the front teeth of the lower jaw for localized pathological abrasion, a - before treatment; b - mouthguard on teeth; c - after treatment.
The mouth guard is made in such a way that in the area of the teeth being reconstructed there is a tight plane contact with the mouth guard, and in the group of separated chewing teeth the gap does not exceed 1 mm (a sheet of writing paper folded in half should pass freely). To monitor and eliminate possible complications after fixing the aligner, the patient is asked to come back the next day, and then asked to come for an appointment as soon as the patient determines the occurrence of tight contact in the group of separated chewing teeth. The patient must first be trained to control the presence of occlusal contact of the teeth by biting a thin strip of writing paper. After reaching contact, the mouthguard is corrected with quick-hardening plastic, achieving disocclusion in the group of chewing teeth up to 1 mm, for which layers of clasp wax plates are laid between the molars. Appointments will be made again once close contact between the separated teeth has been achieved. Thus, using the method of gradual disocclusion, the necessary restructuring of the area of vacate hypertrophy of the alveolar process is achieved.
The method of gradual disocclusion is applicable in the treatment of localized forms of pathological tooth wear without reducing the occlusal height. In the generalized form of this pathology, the method of sequential disocclusion is used. It consists of gradual disocclusion sequentially, first in the frontal area, then on one side in the area of the chewing teeth, then on the other. Considering the long duration of such restructuring, treatment of a generalized form of pathological tooth abrasion without reducing the occlusal height should be considered the most complex and time-consuming with a questionable prognosis, since the disocclusion method does not always achieve the desired result. In addition, it is contraindicated in pathology of the periapical tissues, bone tissue atrophy and in the area of the teeth subject to “restructuring”, diseases of the temporomandibular joint.
The second stage is the restoration of the anatomical shape of worn teeth using one of the previously discussed types of prostheses. The prognosis for the treatment of pathological tooth wear is generally favorable. Treatment results better than the streets young and middle-aged with an initial degree of abrasion. However, it is necessary to note the possibility of relapses in patients with pathological tooth wear due to bruxism and parafunctions, which confirms the idea that only orthopedic interventions are insufficient without appropriate psychoneurological corrections.
All patients with pathological tooth wear should be monitored at the dispensary.
Orthopedic dentistry
Edited by Corresponding Member of the Russian Academy of Medical Sciences, Professor V.N. Kopeikin, Professor M.Z. Mirgazizov
Healthy and beautiful teeth are the main factor in a person’s health, as well as their full existence. It is extremely important that the oral cavity and dentition are always normal. But sometimes it’s quite difficult to keep teeth in good condition throughout his life. Various negative factors - harmful environment, consumption junk food, poor oral hygiene, stressful situations, bad habits - all this can lead to increased wear and tear of teeth. In addition, tooth enamel wears down with age. However, sometimes increased abrasion can be observed at a young age, in these cases you should immediately consult a doctor because this violation indicates various pathological processes in the body.
The process of tooth wear is a common physiological phenomenon. It is observed throughout the life of every person. If there is a correct bite, then the inner part of the upper teeth is erased, and the outer part of the lower teeth wears off. This erasure is considered physiological, and while the human body is still young, it proceeds in a normal manner.
Abrasion of tooth tissue occurs in every person; this occurs as a result of natural physiological function- chewing.
Features of physiological tooth abrasion:
- At the age of 30, the erasing process occurs completely unnoticed, because it is very insignificant. During this period, there is a slight abrasion of the crowns, the tubercles also become a little smaller, and all irregularities are smoothed out. As a result, the crowns of the incisors take on an even and smooth structure;
- By the age of 50, the wear process increases, but the structure of the tooth enamel remains in perfect order;
- At age 50, major changes occur. First, the process of abrasion of the enamel layer to the maximum level is observed, and only after this the dentin is abraded. Sometimes there may be more severe losses.
However, with age, this condition can become pathological. Usually this process is observed at 25 or 30 years of age. This condition may come on suddenly. It is usually classified as a non-carious pathology of the oral cavity.
According to latest research, about 12% of the world's inhabitants are susceptible to pathological wear of the tooth structure. This disorder affects men to a greater extent, almost 63% of cases.
What it is
Increased tooth abrasion is a high abrasion of the structure of the dental tissue. As a result, all this causes a slow decrease in crown height. As a result of this pathological condition, there is an increase in sensitivity, a change in the shape of the crowns, which leads to occlusion of the jaw.
The severity of this pathological process is determined only by the attending dentist. He must conduct an inspection and evaluate general state dentition.

Pathological abrasion of teeth is the result of mechanical, biophysical and chemical effects on the teeth, due to which defects are formed and the height of the teeth decreases.
In addition to the visual inspection, the following procedures must be carried out:
- An impression of the dentition is made. The resulting models must then be carefully studied;
- Electrodiagnostics are carried out;
- Examination using electromyography;
- Orthopantography is done.
Causes
Pathological abrasion of the dentition can be influenced by completely different factors. Therefore, it is worth considering the main reasons that cause this unpleasant process:
- Removal of a unit of dentition, installation of a prosthesis or braces. In this case, an uneven load appears on neighboring and other teeth. For example, when removing molars, the main pressure will be on the area with the canines and incisors;
- The presence of increased tooth wear in cases where there is an abnormal bite or disturbances in the structure of the jaw. For example, with a straight bite, rapid wear of the area with the cutting and lateral edges of the frontal units of the dentition is observed;
- Bruxism.
Attention! This is a disease in which a person is unconscious in night period Grits his teeth. As a result, the enamel structure is destroyed;
- The occurrence of erasure during professional activity. Some professions, namely confectioners, chemists, and factory workers, require people to work in unfavorable conditions. During work, you often have to use various harmful chemicals and materials, particles from which can settle on the surface of the skin, as well as on tooth enamel. All this can speed up the process of enamel destruction;
- Low fabric hardness. In the presence of such unpleasant diseases as hypoplasia, erosion of the enamel structure, wedge-shaped defect or fluorosis, a process of thinning of the enamel structure occurs, and a decrease in the degree of hardness of bone tissue is also observed. As a result, all this causes acceleration of the wear process;
- Various systematic diseases. Metabolic disorder, disorders in endocrine system, as well as the presence of certain pathologies of a specific nature, all this leads to a decrease in the resistance properties of tooth tissue;
- If the diet is poorly regulated, and also if it contains a large number of harmful products. There is a large predominance of solid foods in the menu - apples, carrots, seeds, nuts, and so on. In addition, if the menu contains a large amount of soda, confectionery, sweets, baked goods, sour dishes and drinks. All this causes deterioration of the teeth, reduces their hardness and causes increased abrasion;
- Having bad habits.
Attention! Smoking, drinking alcoholic drinks negatively affects the condition of the bone tissue of the teeth. These factors cause premature abrasion and tooth decay. In addition, bad habits include holding in the mouth various items, opening bottles and cans with your teeth, as well as using them for unsuitable purposes, can lead to cracks, chips on the teeth and premature abrasion;
- The use of certain aggressive drugs. Especially when using medications containing hydrochloric acid;
- Doing heavy physical activity. Often athletes, and sometimes loaders, experience increased tooth wear. This is due to the fact that when lifting heavy weights, these people have to close their teeth tightly.
Classification
Typically, increased abrasion is divided depending on the nature and degree of development of the pathology.
There are several degrees:
- First degree. At this stage of the pathological process, abrasion of the upper layers of the enamel coating of the incisors is observed, while the dentin is not affected;
- Second degree. Complete erasure of the enamel is observed. In addition, all chewing cusps are erased, the structure of the crowns is erased until a layer of dentin appears;
- Third degree. More than half of the crowns are erased. The dental cavity is visible through the row;
- Fourth degree. This is the last stage. In this case, complete abrasion of the crowns of the teeth up to the cervical area occurs.
According to the second classification, this violation is considered depending on the area of erasure:
- Vertical. This species is characterized by abrasion of the outer side of the dental unit. This condition is usually observed with malocclusion;
- Horizontal. The erasing process occurs with a decrease in the height of the crown;
- Mixed. This process is characterized by the combination of two pathological processes of erasure.

Vertical abrasion of tooth enamel is one of the clinical forms of increased tooth abrasion.
Depending on the nature of the course and spread of this disorder, two types are distinguished:
- Local. During this process, only one area of the surface of the dentition is erased;
- Generated. The abrasion process is observed throughout the entire dentition.
Symptoms
This process is usually accompanied by increased abrasion of the upper enamel layer. Subsequently, wear of soft tissues – dentin – is observed.
During dentin release, tissue wear occurs at an accelerated rate. At the same time, places with chips, sharp corners, and gouges appear. All this causes the appearance of various microtraumas of the tongue, mucous membrane, and lips.

Wounds on the tongue can be caused by injury to the mucous membrane by chips, sharp corners, and roughness of the teeth as a result of their increased abrasion.
At the initial stage of this process, the following symptoms are observed:
- The appearance of increased sensitivity of the enamel layer to temperature changes, as well as mechanical and chemical influences;
- There may be acute painful sensations when consuming very hot or cold food or drinks;
- Various sour, spicy, salty foods can cause discomfort;
- Pain may occur when the brush touches the teeth during morning hygiene procedures.
During the appearance of dentin, sensitivity may decrease, and as wear progresses, it increases several times.
With the intensification of this pathological process, shortening of the painter is noted. Patients may experience symptoms of drooping corners of the lips, problems and discomfort in the temporofacial joint. Sometimes there may be problems with hearing and pain in the tongue area.
In addition, there is a change in the bite. This causes problems when chewing or biting food. It happens that all these disorders have a negative impact on the functioning of the digestive system.
During times of increased abrasion, the entire process can eventually result in the tooth being shortened to the neck. In this case, the cavity can be seen through defects in the dentin.
It is especially worth paying attention to the symptoms of workers in hazardous industries:
- When exposed to various chemicals, uniform damage to the enamel occurs;
- The formation of an identical surface is observed, with no fissures;
- The surface of the teeth has a matte tint without plaque or stone;
- Sometimes exposed, smoothed dentin may appear;
- If a person works in the production of hazardous chemical acids, then he often has tooth wear down to the neck;
- Under the influence of harmful acids, roughness may appear, painful sensations, discomfort while chewing.
At the last stage, mobility of the dentition, changes in the position of units and their loss are often observed. Sometimes resorption of hard tissues appears at the dental roots and septa.
Inspection and diagnostics
First of all, it is necessary to assess the general condition of the patient, determine the extent of the pathological process, and carry out diagnostics.
When diagnosing, the dentist performs the following procedures:
- He consults with the patient, collects all medical history data, listens to all his complaints;
- The doctor must find out whether there are factors such as pain, whether increased sensitivity, aesthetic changes as well as functional changes;
- Held visual inspection, in which the proportions of the face are assessed, and the condition of hard tissues and oral mucosa is studied;
- Palpation of soft tissues is done. This will help identify the presence of underlying pathological processes;
- The jaw joint is palpated and auscultated;
- Mandatory computer examination, with the help of which the doctor will be able to study the model of the jaw, determine the shape, as well as the degree and depth of damage to the tooth;
- The use of additional examinations - radiography, consultation with a neurologist, etc.

Regular visits to the dentist will help identify the problem of increased tooth collection on early stage. And accept necessary measures for treatment and prevention.
Treatment
Treatment of this pathological disorder is usually carried out by dentists, as well as a therapist, orthodontist, and orthopedist.
At first therapeutic therapy the first causes of erasure are eliminated. The following procedures are carried out:
- Various dental and systemic pathologies are cured;
- A normal bite is established;
- Changes to dentures or implants;
- Recovering extracted teeth. Artificial crowns are installed on their areas.
Along with treatment, the use of additional medications is prescribed, food additives, vitamins and mineral preparations. All these products will be able to quickly replenish all the necessary components, normalize the intake of calcium, mineral salts, fluorine, and other useful elements for teeth.
Elimination is then performed. Remineralization is used for this. But at the same time, the patient continues to take vitamin preparations and attend physiotherapeutic procedures. Applications are also additionally made, which are based on fluorine-containing components.
All sharp edges, chips, and protrusions must be sanded. They must have a smooth and safe surface for the soft tissues of the oral mucosa and tongue.
If there are defects or gaps in the dentition, correction is carried out using prosthetics and implants.
If there is burxism, then in these cases the doctor prescribes night guards. These components will help protect the fabric from wear and tear during nighttime teeth grinding.

Mouthguard is the most effective way to treat bruxism; night guards prevent the teeth from closing during spasms of the jaw and facial muscles and, as a result, prevent their abrasion.
At the final stage of treatment, the natural shape of the teeth is restored. Various means are used for this:
- Filling materials;
- Stump inlays;
- Veneers;
- Artificial crowns;
- Lumineers;
- Artistic restoration.
Prevention
In order to prevent recurrence or the onset of increased tooth wear, the following important preventive measures should be taken:
- If there is a malocclusion, then it is necessary to consult a doctor in a timely manner to correct this disorder;
- When teeth are removed, dentures must be installed in their place. This will prevent stress on adjacent teeth;
- If there is burxism, then it is necessary to take all possible measures to eliminate this pathology;
- It is imperative to maintain the necessary oral hygiene;
- When working in hazardous industries, use protective equipment;
- It is necessary to take medications prescribed by dentists to strengthen tooth enamel.
It is important to identify pathological abrasion at the very first stage. When the first signs of this disorder appear, you should consult a doctor promptly. It is worth remembering that if you delay, serious dental pathologies may appear, even completely erasing them.
Increased tooth wear is a pathology that requires urgent treatment. Every year this disease becomes “younger”, affecting people under 30 years of age. Intensive loss of hard tissue leads not only to aesthetic problems, but also to functional disorders of the dentofacial apparatus. Why does the disease develop, what treatment methods does modern dentistry offer?
The difference between natural and pathological tooth wear
Throughout life, a person’s enamel gradually wears away - this normal process. It wears off very slowly even in children - this is how the teeth adapt to the chewing load. Normally, the thickness of the enamel decreases only in the area of tooth contact, while the dentin is not affected. Normal is a gradual loss of the hard layers of the tooth by 0.034–0.042 mm per year.
By the age of 30, a person’s front teeth wear down slightly, and the masticatory cusps acquire a smoothed outline. By the age of 50, the enamel on contact surfaces disappears almost completely without damaging other tissues. In older people, dentin begins to wear down. If the described process accelerates, this indicates pathological abrasion of teeth.
Pathology is indicated by a decrease in the thickness of the hard layers of the elements of the dentition in young people - usually the abrasion process begins at 25–30 years of age. In humans, the height of the crown slowly decreases, its shape changes, the bite is disturbed, and the sensitivity of the units increases.
This condition can occur suddenly. Research suggests that 12% of the planet's population is susceptible to this pathological process, and in more than 60% of cases men suffer from the disease.
Classification of pathology

This article talks about typical ways to solve your issues, but each case is unique! If you want to find out from me how to solve your particular problem, ask your question. It's fast and free!
 There is a classification of the process of tooth abrasion, compiled depending on the type and complexity of the disease. There are 4 degrees of abrasion:
There is a classification of the process of tooth abrasion, compiled depending on the type and complexity of the disease. There are 4 degrees of abrasion:
- 1 – reduction in the thickness of the top layer of enamel;
- 2 – complete erasure of the hard layer of the unit down to the dentin;
- 3 – the crown is reduced by more than half, a dental cavity becomes noticeable;
- 4 – the unit is erased to the ground.
Depending on the complexity of the disease, there are:
- local abrasion - only one area of the dentition is affected by pathology;
- generalized - the process spreads to both jaws, but the degree of damage to units may vary.
There is also a classification that determines the plane under which the teeth were abraded:
- horizontal – the height of a person’s crowns decreases almost uniformly;
- vertical – the front surface of the lower parts and the back part are subjected to grinding upper canines and incisors (occurs in malocclusion);
- mixed - teeth are destroyed in both planes.
Tooth wear occurs in various forms, and the severity of each may vary. However, if dentin is affected and the nerve dies, the pathological process is irreversible.
Using the classification, the doctor determines the percentage of enamel loss and the rate at which the disease progresses.
Causes and symptoms of increased abrasion
To understand why a patient develops pathology, the dentist must ask him about his lifestyle and find out about diseases in the family. The most dangerous causes of increased tooth wear are hereditary factors:
- Congenital disorder of hard tissue formation. The disease develops due to a lack of microelements in the mother’s body during pregnancy for the development of the fetus, as well as their deficiency in the first year of the baby’s life.
- Marble disease, osteogenesis and other ailments that are inherited.
- Diseases associated with dysfunction of the thyroid gland and problems with the body's absorption of calcium.
Also, increased tooth wear is provoked by other reasons:
- broken bite;
- night grinding of teeth (bruxism);
- loss of several teeth;
- frequent intoxication of the body due to regular use alcohol and smoking;
- incorrectly performed prosthetics or unsuccessfully installed filling;
- softening of enamel in some diseases;
- frequent consumption of foods containing acid (juices, candies, etc.);
- poor nutrition, including constant use sweet, flour and hard products;
- bad habits - chewing the ends of pens, toothpicks and other objects;
- taking certain medications that lead to the destruction of the hard layers of the tooth;
- work associated with exposure to hazardous work.
 With pathological abrasion in humans, the sensitivity of the enamel to temperature changes increases. Associated signs of the disease:
With pathological abrasion in humans, the sensitivity of the enamel to temperature changes increases. Associated signs of the disease:
- sharp, strong pain, often appearing at night;
- increase in interdental spaces;
- presence of caries;
- reducing the height of the crowns;
- trauma to the mucous membrane due to the formation of chips and sharp edges of the teeth;
- change in bite;
- frequent cheek biting;
- feeling of roughness of teeth;
- feeling of jaws sticking together when closing them;
- change in enamel color.
Treatment of increased tooth wear
If the patient has worn down teeth, treatment is carried out taking into account the severity of the process. The efforts of doctors are aimed at eliminating the causes of abrasion: fighting bad habits, replacing dentures, correcting bites, etc.
 Pathological abrasion of teeth at an early stage is treated using remineralizing therapy - the patient is prescribed vitamin complexes, applications are made with fluoride-containing preparations, and electrophoresis is performed. If there are sharp edges of the teeth, they are ground down, and for bruxism, the use of a night guard is prescribed. However, most often patients consult a doctor when their teeth have already been significantly worn down. In this case, treatment is aimed at restoring the units.
Pathological abrasion of teeth at an early stage is treated using remineralizing therapy - the patient is prescribed vitamin complexes, applications are made with fluoride-containing preparations, and electrophoresis is performed. If there are sharp edges of the teeth, they are ground down, and for bruxism, the use of a night guard is prescribed. However, most often patients consult a doctor when their teeth have already been significantly worn down. In this case, treatment is aimed at restoring the units.
Treatment of pathological wear of incisors, canines or chewing teeth is carried out using various designs. In dentistry the following are used:
- Crowns. Metal ceramics are used to restore significantly damaged units. If a structure of increased strength is required, products made of metal or zirconium dioxide are installed. The restored tooth takes on part of the load, relieving it from its neighbors.
- Ceramic inlays and veneers. If the wear of the front teeth is severe and has reached the dentin, the units are restored with thin plates (we recommend reading:). They are highly aesthetic and natural in appearance.
- Stump inlays. This technique is suitable for significant tooth wear - a pin is installed in the root canal, around which a crown is built up.
- Prosthetics with implants. When in a patient with a problem of increased abrasion, the units are destroyed to the very foundation, they are replaced with artificial material. The festered roots are removed, and a pin is installed in place of the lost element, onto which a crown is placed. The restoration procedure can take up to six months.
Treatment of pathological tooth wear of stages 3 and 4 necessarily begins with the restoration of the bite - the installation of crowns at the initial stage of therapy is prohibited, since they can cause the formation of a malocclusion. Subsequently, the orthopedist makes and installs prostheses from the same materials (we recommend reading:). Violation of this rule may lead to the need to re-correct the bite.
If the cause of the problem is an increased load on the units, experts recommend installing durable prostheses made of metal or zirconium dioxide (see also:). Fragile ceramics, cermets or metal-plastics are not used.
Regardless of the chosen method of restoring units in case of tooth wear, doctors recommend using a mouth guard to reduce the load on the units. The design allows the muscles to get used to the new position of the teeth.
Prevention measures
To prevent abrasion and changes in the shape of teeth, you need to visit the dentist every six months - this will allow you to identify the problem in time. In addition to the preventive examination, it is necessary:
- cure bruxism and correct bite;
- to refuse from bad habits;
- restore deleted and destroyed units in a timely manner;
- Healthy food;
- use vitamin-mineral complexes;
- in hazardous industries, protect teeth with special devices.
(7 rated at 4,71 from 5 )
Increased tooth wear (pathological tooth wear)
What is Increased tooth abrasion (pathological tooth abrasion) -
Pathological abrasion of teeth (increased abrasion of teeth)- a pathology in which there is an intense loss of hard tissue in one, in a group or in all teeth.
Pathological abrasion is observed in 11.8% of people, more often in men (62.5%).
Before the age of 30, increased tooth wear is rare. Over the age of 30, it is observed on average in 18.5% of men and 16.5% of women. Complete abrasion of the chewing cusps of molars and premolars and partial abrasion of the cutting edges of the anterior teeth are more often (62.5%) observed in men. In women, this process occurs much less frequently (22.7%).
When seeking orthopedic help, tooth wear was noted in 4% of patients aged 25-30 years, in 22.7% - from 30 to 40 years, in 35.3% - 40-45 years, in 26% - in 50-60 years and in 12% - over the age of 60 years.
What provokes / Causes of Increased tooth abrasion (pathological tooth abrasion):
Increased tooth wear can occur on all tooth surfaces for many reasons. Before starting treatment, the doctor must diagnose the problem, identify etiological factors and motivate the patient to undergo restorative treatment. Therefore, a comprehensive and consistent clinical examination, collecting complaints and patient history, diagnosis from specialists in related specialties and understanding the possibilities and treatment options.
Causes of pathological tooth wear There may be overload due to loss of teeth, incorrect design of dentures, malocclusions, bruxism, occupational hazards, as well as insufficient hardness of dental tissues (fluorosis, hypoplasia).
With a straight bite, the chewing surfaces of the lateral teeth and the cutting edges of the front teeth are subject to wear. The length of the crowns of the incisors by the age of 35-40 decreases by 1/3-1/2. Severe tooth abrasion is observed when part of the teeth are missing. In particular, in the absence of molars, intensive wear of the incisors and canines is observed, as they are overloaded.
Workers engaged in the production of organic and especially inorganic acids show uniform wear of all groups of teeth. Increased tooth abrasion is also observed in people working in enterprises where there are excess mechanical particles in the air.
Increased tooth wear also occurs when systemic diseases(endocrine disorders, fluorosis, Stainton-Capdepont syndrome), which reduces the resistance of tooth tissue to abrasion.
The daily process of chewing can also contribute to the loss (erasure) of hard tissue.
Pathogenesis (what happens?) during Increased tooth abrasion (pathological tooth abrasion):
At initial manifestations intensive deposition of replacement dentin is noted according to the area of abrasion. With more pronounced abrasion, obturation of the dentinal canals is observed. There are pronounced changes in the pulp: a decrease in the number of odontoblasts, their vacuolization, atrophy.
With 3-4 degrees of abrasion, the tooth cavity is filled with replacement dentin, the pulp is atrophic, and the root canals are difficult to pass.
Symptoms of increased tooth wear (pathological tooth wear):
Classifications of pathological tooth abrasion
Bracco classification
The Bracco classification is the most widely used. He distinguishes 4 degrees of erasure:
1. Erasure of the enamel of the cutting edges and tubercles.
2. Complete erasure of the cusps up to 1/3 of the crown height with exposure of dentin.
3. Reducing the crown height to 2/3.
4. The process spreads to the level of the tooth neck.
Classification by A.L. Grozovsky
A.L. Grozovsky (1946) identifies three clinical forms of increased tooth wear:
1. Horizontal
2. Vertical
3. Mixed
Classification by V.Yu. Kurlyandsky
During the pathological process, V.Yu. Kurlyandsky (1962) distinguishes between localized and generalized forms of increased abrasion.
Classification by M.G. Bushana
One of the most fully reflecting the clinical picture of tooth wear is the classification proposed by M.G. Bhushan (1979). It includes various clinical aspects functional and morphological nature: stage of development, depth, extent, plane of the lesion and functional disorders.
Depth of tooth damage
I degree – complete dentin exposure and shortening that does not reach the equator (within 1/3 of the length of the tooth crown);
II degree – shortening from 1/3 to 2/3 of the crown length;
III degree – shortening of the tooth crown by 2/3 or more
Stage of development
I (physiological) – within the enamel;
II (transitional) – within the enamel and partially dentin;
III (increased) – within dentin
Damage plane
I – horizontal;
II – vertical;
III – mixed
Length of lesion
I – limited (localized);
II – generalized
Classification by A.G. Moldovanova, L.M. Demner
The most modern classification of increased and physiological abrasion permanent teeth can be considered the classification proposed by A.G. Moldovanov, L.M. Demner, (1979). Long-term clinical studies and observations have shown that with an optimal course of physiological abrasion, the natural loss of hard dental tissues per year ranges from 0.034 to 0.042 millimeters.
Studies have also shown that abrasion within the enamel-dentin boundary at the age of 50 years and older with a preserved dentition, in which there are at least 10 pairs of antagonist teeth, is a natural process.
Based on this, the authors came to the conclusion that physiological tooth abrasion has its own forms of abrasion:
1. I form - abrasion of the incisor teeth and smoothing of the cusps of molars and premolars (up to 25-30 years).
2. II form - abrasion within the enamel (up to 45-50 years).
3. III form - abrasion within the enamel-dentin border and partially dentin (50 years and older).
Classification of increased abrasion of hard dental tissues, includes localized and generalized increased abrasion of hard tissues:
1. I degree - within the enamel, partially dentin.
2. II degree - within the main dentin (without transillumination of the tooth cavity).
3. III degree - within the replacement dentin (with translucency of the tooth cavity).
4. IV degree - abrasion of the entire tooth crown.
Forms of abrasion: horizontal, vertical, facet, lattice, stepped, cellular, mixed.
Classification by A.G. Moldovanova
As a result of the research, A.G. Moldovanov (1992) proposed a classification of increased and physiological abrasion of primary (temporary) teeth.
Physiological abrasion of hard tissues of temporary (baby) teeth:
1. By the age of 3-4 years of a child’s life, the teeth of the incisors and the cusps of the canines and molars wear out (I form).
2. By 6 years - abrasion within the enamel layer, up to a point opening of the enamel-dentin border (II form).
3. Over 6 years - abrasion within the dentinal layer of teeth before replacement with permanent teeth (III form).
Increased abrasion of hard tissues of temporary (baby) teeth:
1. Transillumination of the tooth cavity (IV form).
2. Abrasion of the entire tooth crown (V shape).
With pathological abrasion of teeth, abrasion of enamel and dentin is observed, and after dentin is exposed, abrasion occurs more intensely, since dentin is a softer tissue. As a result, sharp edges of the enamel are formed, which often injure the mucous membrane of the cheek and lips. If treatment is not carried out, the wear progresses quickly and the tooth becomes significantly shorter. In such cases, there are signs of a decrease in the lower third of the face: folds at the corners of the mouth, changes in the temporomandibular joint, pain in the temporomandibular joint and tongue, and decreased hearing.
With the initial manifestations of pathological abrasion of teeth, sensitivity to temperature irritations appears, and as the process deepens, pain from chemical and mechanical irritations appears.
As the cusps of the chewing surface wear off with age, the wear on the incisors progresses intensively. The length of the incisor crowns decreases and by the age of 35-40 decreases by 1/3-1/2. Instead of a cutting edge, significant areas are formed on the incisors, in the center of which dentin is visible. Once dentin is exposed, it wears off more intensely than enamel, resulting in the formation of sharp edges that injure the cheeks and lips. If treatment is not carried out, tissue abrasion progresses rapidly, and the crowns of the teeth become significantly shorter. The lower third of the face decreases, which is manifested by the formation of folds at the corners of the mouth. In persons with a significant decrease in bite, changes in the temporomandibular joint may occur and, as a result, burning or pain in the mucous membrane, hearing loss and other symptoms characteristic of low bite syndrome may occur. With further progression of the process, the abrasion of the incisors reaches the necks. The tooth cavity is visible through the dentin, but it is not opened due to the deposition of replacement dentin. In a deep bite, the labial surface of the lower incisors is in contact with the palatal surface of the incisors upper jaw and these surfaces wear down significantly. The most pronounced tissue abrasion is observed in the absence of part of the teeth. For example, in the absence of molars, on which the relationship of the dentition normally depends, the incisors and canines are intensively worn out, as they are overloaded. In addition, due to overload, displacement of teeth and resorption of bone tissue at the apexes of roots and interdental septa may occur. Often, tooth wear is caused by improper design of removable and fixed dentures. When using a tooth under a clasp without an artificial crown, the enamel and dentin at the neck are often erased. As a rule, patients complain of severe pain when exposed to mechanical and chemical stimuli. As is known, the specific conditions of some industries are the cause of occupational diseases. In a number of industries, teeth are damaged and frequently worn out. In workers engaged in the production of organic and, especially, inorganic acids, examination reveals more or less uniform abrasion of teeth of all groups; there are no sharp edges. The surfaces of the teeth have a matte tint, there is no plaque. In some places exposed dense smooth dentin is visible. In people with extensive experience working in acid production enterprises, the teeth are worn down to the neck. One of the first signs of enamel abrasion under the influence of acid is a feeling of teeth on edge, roughness of the surface of the teeth. The change from a feeling of soreness to pain indicates the progression of the process. The chewing process may be disrupted. Upon examination, a loss of the natural color of the tooth enamel is revealed, which is especially visible when dried. The waviness of the enamel surface may be slightly expressed. Individuals working in enterprises where the air contains excess mechanical particles also experience increased tooth wear.
Often, increased tooth abrasion occurs in a number of endocrine disorders - dysfunction of the thyroid, parathyroid glands, pituitary gland, etc. The abrasion mechanism in this case is due to a decrease in the structural resistance of tissues. In particular, increased abrasion is found in fluorosis, marble disease, Capdepont-Stainton syndrome, primary underdevelopment of enamel and dentin.
Diagnosis of increased tooth abrasion (pathological tooth abrasion):
Before carrying out any treatment, it is mandatory correct diagnosis and interpretation of the existing problem.
The Encyclopedia Americana defines diagnosis as “the art of determining the nature of a disease.” In addition, “a diagnosis can only be made after carefully determining the cause of the pain and performing various tests.”
Dental diagnosis carried out by a doctor requires an assessment of all objective and subjective symptoms, clarification of the cause of the disease and possible associated effects. In addition, a treatment plan is developed based on the medical and dental histories, as well as the data collected from the anamnesis.
In order to accomplish this, a comprehensive and detailed examination of each patient is required. This examination also includes studying the condition of the temporomandibular joint (TMJ), masticatory muscles in function and at rest, the condition of periodontal tissues and occlusion, as well as clinical assessment teeth and aesthetics.
The examination should be conducted in such a way as to increase the patient's awareness of oral health and upcoming treatment, as well as to develop a positive relationship between the doctor, medical staff and the patient. This typically results in the patient developing trust and confidence in the dental team and practice, as well as acceptance and understanding of the required treatment plan. In his book on comprehensive dental diagnostics, Polansky noted: “Many patients have difficulty formulating their complaints. The examination serves as a way to solve this difficult problem, as it helps patients gradually and consistently understand and evaluate their problems.”
Clinical examination
Attrition (loss of hard tissue) can occur on any tooth surface. It most often occurs on the occlusal and vestibular surfaces, but can also be observed on interdental surfaces and the root of the tooth (for example, external and internal resorption). The resorption process has not been well studied in both primary and permanent teeth, but, nevertheless, with the right approach it can be successfully eliminated. Cervical hard tissue loss (vestibular and oral)
Cervical defects can vary in their appearance and have different surface structures. In their latest paper on this issue, Rees et al. indicate: “It is very difficult to single out one etiological factor for such lesions based only on clinical diagnostics. They probably have a multifactorial origin." Very often, not one, but several factors lead to the occurrence and progression of hard tissue loss in the cervical region.
To determine the feasibility and treatment, the following parameters should be clarified:
- Does the patient have any pain symptoms?
- Does tissue loss (occlusal wear) cause functional problems?
- Does tissue loss (occlusal wear) cause aesthetic problems?
Problems often overlap, and the decision about the need for treatment must be carefully considered, using additional diagnostics.
The treatment plan must be comprehensive, providing solutions to all problems associated with the condition of increased abrasion. During the examination, the patient should be informed about the consequences that may occur in the absence of adequate treatment, risk factors, and possible treatment plans should be proposed. The more information the dentist and patient have about the current condition and possible future, the easier it will be to decide when and how to restore.
Carrying out additional diagnostics
Carrying out complex and additional diagnostics - perfect time for the dentist to understand the patient’s problems and motivate him for restorative treatment. As described earlier, the process begins with interviewing the patient. By asking direct and understandable questions, the dentist begins to understand the patient. Each patient is individual, because everyone is raised and trained in a different environment, and this should be kept in mind all the time.
During the examination, the patient should be asked to carefully look, listen and understand what is happening to his teeth. The use of a speculum, intraoral camera, diagnostic models and diagnostic wax-up facilitates the communication process. The patients of 2007 are different from the patients of 1975; they have clear, definite desires for their teeth and know what to do with them. Thanks to media influence and other factors, many patients are more aware of what they want and don't want than they were 30 years ago. Sometimes it is possible to restore the occlusion and satisfy the patient's aesthetic requirements, sometimes it is not the best option to cover with veneers or crowns to achieve a certain "look".
All of these factors must be discussed honestly with the patient for appropriate treatment planning. Christensen said: “Excessive 'treatment' of a patient under the guise of cosmetic dentistry without the patient's informed consent is primarily intended to satisfy the dentist's financial goals. And is nothing more than the worst form of lying." The decision to perform restorative treatment for functional or aesthetic reasons must be made based on the patient's interests and benefits.
When a patient is indicated for restorative treatment, diagnostic models cast into the articulator and preliminary wax-up can be demonstrated. Demonstration of such diagnostic tools to the patient allows one to focus on the scope medical care, necessary to recreate a new occlusion. The details of the explanation of treatment options depend on the nature of the patient: some will require explanations of the smallest subtleties and nuances, while others prefer not to delve into these details. The difficulty is how to present the information to the patient. The decision depends on the doctor’s ability to communicate with the patient, focusing on his level of understanding.
Treatment of increased tooth wear (pathological tooth wear):
Treatment for increased abrasion (loss of hard tissue) can vary depending on the type and nature of the pathology, as well as the skill, skill, and clinical judgment of the physician. The most important factor: conducting as much accurate diagnosis, correcting problems that cause excessive wear, and providing restorative treatment using direct and indirect restorative techniques to restore the patient's mouth to its ideal state of form, function and esthetics.
The physician selects a treatment option, usually based on some philosophy of occlusion such as centric relation, neuromuscular, gnathology, and others. Some dentists prefer a very conservative approach to treatment, while others take the opposite view. The purpose of this article is not to describe dogmas and guidelines about what will or will not work in a particular case. However, here we will describe treatment methods that the author of the article successfully applies, and this is confirmed by literature data. The following treatment options correspond to all types of occlusal philosophy:
1. Identification and elimination of etiological factors. The first issue that must be addressed in restorative treatment, regardless of whether we are talking about non-carious cervical lesions or increased occlusal wear, is the identification of etiological factors and their elimination. In many cases, after casting the models into a semi-custom articulator, the dentist can identify certain relationships between the upper and lower dental arches that are preventing smooth protrusive and lateral movements. This can be corrected in several ways, depending on the overall treatment plan. If the treatment does not involve modification of the occlusal surfaces by covering with onlays or crowns, then conservative selective grinding may help. Dawson stated: "Occlusal balance involves the correction of the occlusal contact points upon which the excessive load, by selective grinding. This involves selectively reshaping the surface of the teeth to ensure normal jaw function.” It should be noted that “occlusal balance” implies not only the removal of tooth tissue, but also, in some cases, the addition of restorative material to some surfaces to create the most optimal occlusal plane. The goal is to remove areas of increased stress that result from increased wear, causing pain in the patient and preventing free movement of the jaw.
2. Proper restoration of lost tooth tissue. The second prerequisite is the restoration or replacement of lost hard tissues. This can of course be done using various methods and technologies and again depends on the experience of the dentist and the wishes of the patient. For example, carious and non-carious cervical lesions can be restored using composite material, glass ionomer cement, amalgam, gold foil or cast gold inlay. The decision is usually made based on durability, availability, price and aesthetics. When large occlusal changes or morphological changes are planned, crown closure may be chosen as a treatment option. The type of crown is determined by clinical indications. A cast gold crown is the standard and has the greatest durability, but all-ceramic crowns are just as good, according to recent data. Therefore, in many cases, all-ceramic crowns can be used as a treatment option as well as metal-ceramic crowns, with equal success rates, as long as occlusal and other factors are taken into account and understood.
3. Maintaining occlusal relationships. Finally, the dentist must help the patient maintain the resulting occlusal relationship for as long as possible. This is helped by an individually designed prevention program, including professional hygiene, during which the condition of periodontal tissues and restoration structures is monitored. Very often, an occlusal guard helps preserve restorations by keeping increased loads at night or during the day to a minimum. The occlusal guard must be balanced intraorally in all positions of the jaw.
Increased abrasion with loss of hard tissue changes the condition of a person’s dentition. It manifests itself in varying degrees of severity at different periods of life and in some cases leads to loss of function and aesthetics and the occurrence of pain symptoms. The article discusses possible reasons erasures and treatment options, with an emphasis on patient education and diagnosis. The author’s task: to draw the attention of doctors to this problem in order to further increase the level of knowledge and skills for the functional and aesthetic correction of this condition.
Prevention of increased tooth abrasion (pathological tooth abrasion):
Prevention of pathological tooth abrasion comes down to eliminating the factors leading to tooth wear: timely prosthetics, the use of respirator masks in the production of abrasive substances, rinsing with a soda solution in the production of acids.
Which doctors should you contact if you have increased tooth wear (pathological tooth wear):
Is something bothering you? Do you want to find out more detailed information about Increased tooth abrasion (pathological wear of teeth), its causes, symptoms, methods of treatment and prevention, the course of the disease and diet after it? Or do you need an inspection? You can make an appointment with a doctor– clinic Euro Be sure to take their results to a doctor for consultation. If the studies have not been performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You? It is necessary to take a very careful approach to your overall health. People don't pay enough attention symptoms of diseases and do not realize that these diseases can be life-threatening. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. Each disease has its own specific symptoms, characteristic external manifestations- so called symptoms of the disease. Identifying symptoms is the first step in diagnosing diseases in general. To do this, you just need to do it several times a year. be examined by a doctor to not only prevent a terrible disease, but also maintain healthy mind in the body and the organism as a whole.
If you want to ask a doctor a question, use the online consultation section Glossitis (inflammation of the tongue)
If you are interested in any other types of diseases and groups of human diseases, or you have any other questions or suggestions, write to us, we will definitely try to help you.