Muscle and bone infections. Diseases of the muscular system. Cellular structure of bones
Skeletal muscles provide all movements associated with walking, eating and labor processes. A person has about 600 pairs of them, and they make up almost 40% of his body weight. There are 222 bones and approximately 206 joints in the human body.
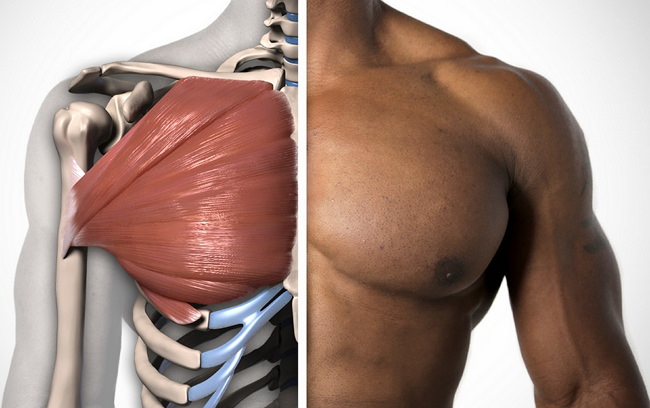
The musculoskeletal system performs the musculoskeletal function. It consists of a skeleton, the bones of which serve as levers, and striated muscles attached to the bones, which act as a power unit. The skeleton consists of bones and their joints. It performs the functions of support, movement and protection. The supporting function is manifested in the fact that the skeleton supports other organs, gives the body a constant shape and allows it to take certain positions. Skeletal bones, within certain limits, provide protection for internal vitals. important organs from external rough physical influences. So, the brain is located in the cranium, and the spinal cord is in the spinal canal, bones chest protect the heart, lungs and other organs located in it, and the pelvic bones protect the organs of the genitourinary system. According to their shape, all bones are divided into long ones ( tubular bones limbs), short (vertebrae, heel bone) and flat (scapula, ribs, pelvic bones). All bones are covered with periosteum, which is a connective tissue plate tightly fused with the bone. From it, nerve fibers and vessels penetrate the bone and provide metabolic processes. Special cells of the periosteum - osteoblasts - are involved in the formation of bone tissue, both during its growth and during healing after fractures.
5. Circulatory system. Structure and functions.
The circulatory system is a system of vessels and cavities through which blood circulates. Through circulatory system The cells and tissues of the body are supplied with nutrients and oxygen and are freed from metabolic products. Therefore, the circulatory system is sometimes called the transport, or distribution, system.
Blood vessels are divided into arteries, arterioles, capillaries, venules and veins. Arteries carry blood from the heart to the tissues. Along the blood flow, the arteries branch into trees into more and more small vessels and turn into arterioles, which in turn break up into a system of the finest vessels - capillaries. The capillaries have a lumen almost equal to the diameter of the red blood cells (about 8 microns). Venules begin from the capillaries, which merge into veins that gradually enlarge. Blood flows to the heart through the largest veins.
There are two circles of blood circulation - large and small.
The pulmonary circulation begins with the pulmonary trunk, which arises from the right ventricle. It delivers blood to the pulmonary capillary system. Arterial blood flows from the lungs through four veins flowing into left atrium. The pulmonary circulation ends here.
The human body is an integral system, which includes cells, tissues and organs. The latter are combined with each other to perform important functions. One of the main ones is the human skeletal system, which we will get acquainted with in more detail. Let's consider pathologies and their treatment.
What is included in the skeletal system?
The human skeletal system provides the framework or support for the entire body. It's hard to imagine what a person would look like without it. It, in turn, consists of individual components that work as a whole. Elements include:
All these organs of the skeletal system are a kind of bricks from which it is built
Functions of the musculoskeletal system
All organs that belong to it collectively perform the following functions:
- This is the support of our body.
- Provides strength and rigidity.
- Movement function.
- Hematopoiesis and accumulation of minerals.
- Protection of vital organs.
It is the skeletal system, together with the muscles, that gives the human body its appearance. Unfortunately, there are situations when it cannot cope with its functions 100%. Some pathological conditions develop that disrupt its functioning. Diseases musculoskeletal system are now quite common. There are quite a lot of reasons that can be given.
What provokes and muscles
Currently, doctors cannot name the exact cause of the development of a particular disease. We can only assume that most often the cause of such pathologies are:

The same disease in different patients can be caused by for various reasons, which are established during the examination of the patient.
How do diseases of the skeletal system manifest themselves?
Everyone’s body is different and does not react the same way to certain problems, so the symptoms of such pathologies are quite diverse. Most often, diseases of the skeletal and muscular systems are manifested by the following symptoms:

The course of the disease has a great influence on the symptoms. There are diseases of the skeletal system that proceed almost unnoticed and progress rather slowly, which means that the symptoms will be mild. And the acute onset of the disease will immediately make itself felt with obvious signs.
Groups of diseases of the skeletal system
All diseases of the human musculoskeletal system can be divided into several groups:
- Traumatic pathologies. This group is the most understandable, as it arises under mechanical influence external factors. If you consult a doctor in a timely manner, the therapy is successful and no complications arise.
- Diseases inflammatory in nature. They may develop as a result of injury or infectious process. They are divided into purulent and tuberculous.
- Dystrophic diseases. They are most often provoked by disturbances in metabolic processes, but can be caused by errors in nutrition and the influence of external factors. A striking example is rickets.
- Dysplastic diseases are manifested by disturbances in the shape of bones, which leads to changes in the human skeleton. The cause of such pathologies is often birth trauma or hereditary predisposition.
It should be noted that the skeletal system also suffers from pathologies that can be classified into several groups. A combination of different symptoms may be observed.
Pathologies of the skeletal system
Despite all its strength, the skeletal system is quite vulnerable to various kinds influences. There are many reasons that can provoke diseases. Some patients are forced to struggle with such pathologies due to hereditary disorders, while others acquire them during their lives.
Let's look at some of the most common diseases:

This is just a small list of diseases of the skeletal system. But you need to know that even hereditary pathologies can now be corrected and it is possible to improve the patient’s quality of life.
Diseases of the muscular system
Muscles are an integral part of the musculoskeletal motor system, so their diseases also lead to various violations throughout the body. Here is a list of the most common pathologies:

Joint pathologies
The skeletal system provides us with active movements due to the presence of joints, that is, movable bone joints. Diseases of these formations can be associated with various processes:

The lining of the joint, as well as cartilage tissue, can become a source of tumor.
There are various diseases of the musculoskeletal system, but among them osteoarthritis is more common than others. It may be idiopathic in nature or develop against the background of other diseases, for example, with disorders of the endocrine glands.
The joints of the lower extremities are most often affected, less often the upper ones. The pathological process can involve several joints at once. The earlier the disease is detected, the more efficient process treatment.
Areas of therapy for diseases of the skeletal system
As you know, the treatment of any disease requires integrated approach. This is the only way to quickly and effectively cope with pathology. The same, undoubtedly, can be attributed to the human musculoskeletal system.
Treatment of the skeletal system is most often carried out in several directions:
- Drug therapy.
- Adequate physical activity.
- Physiotherapeutic procedures.
- Traditional methods of treatment.
- Adjusting your diet.
An important role in the treatment of diseases of the musculoskeletal system is played by the patient’s attitude towards his health. If the patient relies only on medications and does not want to change his diet and lifestyle, then effective treatment will not work.
Drug therapy
As a rule, the skeletal system of the body almost always signals its diseases. painful sensations. Since the cause may be inflammatory processes, therapy usually begins with the prescription of medications:
- "Diclofenac".
- "Ibuprofen."
- "Ketorolac".
- "Naproxen."
- "Celocoxib".
For pathologies of the musculoskeletal system, doctors recommend taking medications containing glucosamine and chondroitin, which have a good effect on cartilage tissue and promote its restoration.
If there is infectious nature illness, then you can’t do without antibacterial drugs and corticosteroids.
Therapeutic massage against diseases of bones and muscles
If the musculoskeletal system fails, long-term and complex treatment will be required. Not last place occupies a role in therapy Since ancient times, healers have known its healing power.
Massage affects not only a certain area, but also the entire body as a whole. The interaction between systems and organs is normalized, which leads to the disappearance of pathologies and general improvement.

The benefits of massage for diseases of the musculoskeletal system are as follows:
- Muscle tone is normalized.
- Tissue nutrition improves due to normalization of blood circulation.
- Motor functions are restored.
- The pain of damaged areas is reduced.
- Lymph flow improves, which stimulates metabolic processes in tissues.
- Massage does not allow muscles to atrophy.
- Only with the help of massage can you get rid of hematomas, which often appear in the injured area.
Despite this miraculous effect of massage, there are also contraindications to this procedure, so before visiting a massage therapist, it is advisable to discuss this issue with your doctor.
Traditional methods of treating diseases of the skeletal system
In the bins of traditional healers there are quite a lot of recipes for treating diseases of the joints and muscles. Here are some that you can use at home:
- Onion ointment is great for pain in the joints and back. To prepare it, you need to chop 5 onions in a blender, add 8 tbsp. l. vegetable oil, three tablespoons of beeswax. Saute this entire mixture until the onions acquire a golden color, about 45 minutes. After this, squeeze out the liquid and can be used by rubbing into the joints and lower back. Keep refrigerated.
- Traditional healers claim that Bay leaf copes well with osteochondrosis. You need to fill one and a half packs with a glass of water and boil for 5 minutes. Leave for three hours and throughout the day in small portions accept. Getting ready every day new line-up. Take 3 days, then rest for 7 days and repeat.
- With the help of ginger, you can reduce inflammation in the joints or prevent it altogether in case of arthritis. Drink like regular tea or you can add ginger to salads and soups.
Traditional recipes can only be used as an addition to the main course of treatment. You should not take them without consulting your doctor, as some medications may be incompatible with herbs.
How to prevent the development of diseases of the musculoskeletal system
Of course, it is clear that if there is a hereditary pathology, then nothing can be done, but acquired diseases can be prevented if you follow some recommendations:
- News active image life, there must be daily stress on bones and muscles.
- Alternation of work and rest.
- Every day walk and walk in the fresh air.
- Introduce more foods containing calcium and silicon into your diet.
- Drinking enough water.
To summarize, our skeletal system needs movement, healthy image life, right and balanced diet and enough water. It is always worth remembering that it is much easier to acquire a disease than to get rid of it later, so you need to take care of your health from a young age.
Man is a vertebrate whose closest relative is the monkey. The life activity systems of these two biological species are very similar; however, as a result of the acquisition of new evolutionary skills, which include upright walking, the human body has acquired only its own characteristics.
In particular, this affected the musculoskeletal system (MS): the human chest is flatter, the pelvis has become wider, the length of the lower extremities has exceeded the length of the upper, the volume of the head part of the skull has increased, and the facial part has decreased.
The musculoskeletal system consists of movable and fixed bone joints, muscles, fascia, ligaments, tendons and other connective tissues necessary to perform locomotor (motor), support and protective functions.
It includes over 200 bones, about 640 muscles and many tendons.
The central nervous system (CNS) regulates the activity of the central nervous system.
Vital organs are protected by bone structures. The most protected organ, the brain, is located in a “box” sealed from the outside - the skull. Spinal canal protects the spinal cord, the chest - the respiratory organs.
Functions of ODS
Supportive, protective and motor - these are the three most important functions of the musculoskeletal system that form the body of any vertebrate, without which it cannot exist.
But besides them, the musculoskeletal system also performs the following functions:
- softening, spring sudden movements and vibrations;
- hematopoietic;
- metabolic (metabolic) - exchange of calcium, iron, phosphorus, copper, important mineral elements;
- biological - provision important processes vital functions (circulation, hematopoiesis and metabolism).
The versatility of the ODS is caused by the complex structure and composition of bones, their strength, and at the same time lightness and elasticity, the presence of various types of connections between bones (articular, cartilaginous and rigid).
Bone is the cornerstone element of the musculoskeletal system
Bone is a solid living organ in which continuous processes occur:
- bone formation and resorption (destruction of bone tissue);
- production of red and white blood cells;
- accumulation of minerals, salts, water, organic compounds.
Bone has the ability to grow, change and regenerate. So, a small, newly born child has over 270 bones, and an adult has about 206. This is due to the fact that as they grow, many bones lose cartilage and fuse together.
Bone composition
The bones of the musculoskeletal system include the following elements:
- periosteum - outer layer of connective tissue;
- endosteum - an internal connective tissue layer that forms the medullary canal inside the tubular bones;
- bone marrow is the soft tissue substance inside the bone;
- nerves and blood vessels;
- cartilage.
All bones are composed of organic (mainly collagen) and inorganic elements. The younger the body, the more organic compounds there are in the bones. In an adult, the collagen content in bones drops to 30%.
Bone structure
In terms of structure, bone under a microscope looks like a collection of concentric layers - plates inserted into each other, consisting of protein, mineral matter(hydroxyopatite) and collagen. This structural unit is called an osteon. The inner plate forms the so-called Haversian canal - a conductor for nerves and blood vessels. In total, an osteon can contain up to 20 similar plates, between which there are asterisk-like plates bone cells. There are also insert plates between the osteons themselves. The lamellar structure, penetrated by the neurovascular Haversian canals, is characteristic of all bone surfaces, both external and internal, except for spongy bones. The presence of channels promotes the active participation of bones in mineral and bone metabolism and hematopoiesis (blood formation).
Cellular structure of bones
There are three types of cells in bones:
- Osteoblasts are immature young bone cells that synthesize the matrix - intercellular substance. They form on the surface of growing bones, as well as in places of bone damage. Over time, osteoblasts become cemented in the matrix and transform into osteocytes. These are the main participants in osteogenesis (bone synthesis).
- Osteocytes are mature, non-dividing, almost non-matrix-producing cells that communicate with each other through the channels of the cavities (lacunae) in which they are located. Tissue fluid circulates between the processes of osteocytes, its movement occurs due to the vibration of osteocytes. Osteocytes are living cells - thanks to them, metabolism is carried out and the mineral and organic balance in the bones is maintained.
- Osteoclasts are huge multinucleated cells that destroy old bone tissue. They, too, like osteoblasts, are important participants in bone formation. A balance must be maintained between osteoblasts and osteoclasts: if there are more osteoclasts than osteoblasts, osteoporosis begins in the bones.
Most bones develop from cartilage tissue, except for the bones of the skull, lower jaw and, presumably, the collarbone - they are formed from connective tissue.

Types of bones
The human musculoskeletal system is represented by bones of various types - long, flat, short, mixed, sesamoid.
- Long tubular bones have a rounded, hollow shape when cut. The middle elongated part of the bone (diaphysis) is filled inside with yellow bone marrow. At both ends of the tubular bone there is a head (epiphysis), covered on top with hyaline cartilage, and inside consisting of a spongy substance that contains red bone marrow. The growing part of the bone (metaphysis) is the area between the epiphysis and diaphysis. In children and adolescents, the metaphysis consists of cartilage, which is replaced by bone at the end of growth. The long tubular bones include the bones of the limbs, in particular the longest one, the femur.
- Flat bones are non-hollow, have a thin cut and consist of a spongy substance, covered on top with a compact smooth layer. The scapula, pelvic bones, and ribs have this structure.
- Short bones have a tubular or flattened structure, but there is no single cavity inside them. Cells with bone red marrow are separated by partitions. The short bones include the phalanges of the fingers, the carpus, the metacarpus, the tarsus, and the metatarsus.
- Mixed bones can combine elements of flat and short bones. Mixed bones include the vertebrae, occipital and temporal bones of the skull.
- Sesamoid bones are located deep in the tendon, at the point where it passes through the joint (knee, wrist, foot, etc.), they usually lie on the surface of another bone. Their task is to protect the tendon and strengthen the muscle by increasing the power arm.
All bones have irregularities in the form of protrusions, tubercles, depressions, and grooves. This is necessary for connecting bones and attaching muscle tendons.
A few notes about bone marrow
The bone marrow, unlike the brain and spinal marrow, has nothing to do with the central nervous system; it does not have neurons. This - hematopoietic organ, consisting of myeloid two-component tissue (stroma + hemal component).
In the growing bones of the skull and facial bones, mucous bone marrow is formed - a gelatinous consistency depleted of cells.
Main components of the human skeleton
The skeleton is the static basis of the human musculoskeletal system. The construction of the whole body begins with it. Skeletal anatomy must be adapted to each organ individually and to the entire set of vital systems, providing all the necessary functions of the musculoskeletal system.
Human skull
Let's start with the part that crowns the skeleton - the skull.
Humans are the highest mammals in the evolutionary chain, and this is reflected in our skull. The volume of the adult human brain is about 1500 cubic centimeters, so the brain portion of the human skull is relatively larger than that of animals. Relatively - this is in comparison with front part. The human lifestyle inevitably led to the fact that in the process of evolution, people's brains grew and their jaws became smaller, because man, having learned to use tools, abandoned raw food.
The brain part of the skull consists of four unpaired and two paired bones fused together:
- unpaired - frontal, sphenoid, ethmoid and occipital;
- paired - two temporal and two parietal.
All the bones of the brain part of the adult skull are connected motionlessly, but in a newborn the sutures remain uncovered for a long time, connecting to each other through “fontanelles” - soft cartilaginous tissue - this is how nature took care of the growth of the skull.
In the occipital part of the skull there is an opening connecting the brain and the spinal cord; arteries supplying the brain with blood also pass through it. The skull is attached to the spine using an elliptical joint. Mobility is ensured by the first two cervical vertebrae, called atlas and epistropheus.
The facial part includes the following bones:
- paired bones: facial jaw, cheekbones, nasal bones, nasal cavity bones, palate;
- unpaired bones: lower jaw, hyoid bone, vomer.
The lower jaw is the only movable articular joint of the skull, and where there is a joint, there are diseases such as arthritis, dislocation, osteonecrosis, etc.
The spine is the basis of the ODS
The spine is the axial rod of the human motor system. Unlike animals, he has vertical position, which is also reflected in its structure: in profile, the spine in humans looks like the Latin letter S. These natural curves of the spine are designed to counteract the compressive forces to which the vertebrae are continuously exposed. They play the role of shock absorbers and balance the spine when dynamic load increases.

If there were no bends, our spine could break during a normal jump and it would be difficult to maintain balance.
There are five in total in the spine vertebral sections and up to 34 vertebrae (maybe a couple less due to the different number of vertebrae in different people in the rudiment of the tail - the coccyx).
- the cervical spine has 7 vertebrae;
- chest - 12;
- lumbar and sacral - five vertebrae each;
- coccygeal - from 3 to 5.
Distribution of curves in the spine
The curvatures of the spine in adjacent sections are oppositely directed:
- cervical spine - the bend is directed forward, it is called lordosis.
- thoracic region - the bend is directed backwards, this is kyphosis. Exceeding the norm is called stooping.
- lumbar region - lordosis;
- sacral region - kyphosis.
Excessive bending in the lumbosacral region can lead to displacement of the vertebrae (spondylolisthesis), hernia, and destabilization of the spinal column.
The flexibility of the spinal column is also controlled by the vertebrae, which are semi-movably connected to each other using cartilaginous plates - intervertebral discs. Dystrophic changes in the discs lead to a catastrophic disease - osteochondrosis, from which all other orthopedic pathologies originate.
Let us now consider the remaining large elements included in the ODS.
The musculoskeletal system includes such important parts of the skeleton as the chest, shoulder girdle, upper and lower limbs, and pelvic girdle.
Rib cage
The chest is the storage area for organs chest cavity(heart, trachea, lungs). It is reinforced with a rib frame of 12 pairs of ribs:
- The first 7 pairs in front are semi-movably attached to the sternum;
- The 8th, 9th and 10th pairs of ribs are connected to each other by cartilage;
- the last two pairs are free.
At the back, all the ribs and vertebrae articulate, forming the costoarticular joint.
The thoracic region is inactive, so osteochondrosis in the chest is quite rare, but joint blockage, arthrosis, and intercostal neuralgia can be frequent sources of pain here.
Shoulder girdle
The shoulder girdle consists of two wedge-shaped shoulder blades and two curved clavicular bones, connecting in front to the sternum and behind to the shoulder blades. TO shoulder girdle upper limb tied. Shoulder joint the loosest joint in the human body - this determines multidimensional free movement of the arm, but at the same time it threatens with problems such as shoulder dislocation, glenohumeral periarthritis, etc.
Upper limbs
Everyone seems to know what the upper limbs are made of, but anatomical terms do not always coincide with people’s definitions: many people call the collarbone the shoulder, and the upper arm the forearm. In fact, the hand consists of:
- from the humerus (the upper part of the arm that fits into the shoulder joint);
- the forearm, which includes two bones - the ulna and radius;
- carpal bone.
The hand has a lot of small bones:
- the wrist consists of eight bones, seven of which are arranged in two rows;
- metacarpus - made of 5 bones;
- fingers - from phalanges (two per thumbs, three in the rest).
Such a terrible disease as rheumatoid arthritis begins precisely in the small wrist joints, so they can be a good indicator of this pathology.
Pelvic girdle
Located approximately in the middle of the body skeleton, the pelvic girdle plays an important role in distributing all loads on the spine (the center of gravity of the body is located just above it) and in balancing the spine. In addition, the pelvis protects important organs of the genitourinary system. Through the caudal foramen at the bottom, the hip and pelvis joint is attached to the spine.
The pelvic girdle consists of fused paired bones - the ilium, ischium and pubis. Hip joint (HJ) - from acetabulum(recesses in ilium) and the head of the femur.
Problems with the hip joint that lead to disability are coxarthrosis and hip dislocation. In addition, there are congenital anomalies associated with displacements and underdevelopment of the pelvic bones, leading to severe forms scoliosis.
Lower limbs
The lower limbs include the femur and tibia (tibia and fibula) and feet, connected by the knee joints.
Foot composition:
- seven bones of the forearm, of which the calcaneus is the largest;
- five metacarpal bones;
- 14 phalanges of fingers (two in the big ones, three in all the others).
The knee joint, as well as the ankle, are the most loaded joints in the human body, so arthrosis, tendonitis, heel spurs, sprains and ligament tears make up the lion's share of problems with the lower extremities.
Muscle structure of the ODS
The musculoskeletal system also includes muscles: they are inextricably linked with the skeleton, without them it would simply collapse into a pile of bones. They are also not only a holding force, but also an active driving force.
Muscles consist of elastic tissue, microscopically represented by muscle cells - myocytes.
Muscle types
There are three types of muscles:
- skeletal or striated;
- smooth;
- cardiac.
The movement of absolutely all parts of our skeleton, including facial expressions, is carried out precisely by striated muscles. Skeletal muscles make up the majority of all muscles - there are more than 600 of them, and the total relative weight in the human body is about 40%. The smoothness and coordination of all movements is created due to the presence of agonist and antagonist muscles, which create two multidirectional efforts: the agonists perform the movement, the antagonists resist it.

The motor function of skeletal muscles is caused by their ability to contract in response to a signal from a nerve impulse coming from the central nervous system. The work of the muscles of this group is completely subject to the control of the human brain.
Striated muscles are 70-80% water, and the remaining 20% are proteins, glycogen, phosphoglycerides, cholesterol and other substances.
The most-most muscles of the body:
- The calf and chewing muscles are recognized as the strongest.
- The largest is the gluteal;
- The smallest are the ears;
- The longest muscle is the sartorius muscle, stretching from the ilium to the tibia.
Smooth muscle is a tissue that is part of all internal organs, skin and blood vessels. Spindle-shaped muscle cells make slow movements, not subject to the will and control of a person - they are controlled only by the vegetative nervous system(VNS). Without smooth muscles, digestion, blood circulation, and work are impossible. Bladder and other life processes.
The cardiac muscle is included in a separate group, since it is striated, and at the same time it is not subordinate to human consciousness, but is subordinate only to the ANS. Also unique is the ability of the muscle to contract when removed from the chest cavity.
Muscle classification
There are a lot of muscles in the human body. They can be combined into separate groups according to their functions, the direction of the fibers, their relationship to the joints and their shape. Let's summarize the classification in a table:
| Classification type | Muscle names |
| By function: | Flexors, extensors, adductors, abductors, rotators, erectors, elevators, depressors, sphincters and dilators, synergists and antagonists |
| By fiber direction: | Rectus, transverse, teres, oblique (unipennate, bipennate, multipennate, semitendinous, semimembranosus) |
| In relation to joints: | One-piece, two-piece, multi-piece |
| By form: | Simple:
|
The human musculoskeletal system is a complex symbiosis different systems: bone, muscle, nervous, vegetative. It is inextricably linked with a person; any life process depends on it. It is designed simply beautifully, developing with us. There is nothing superfluous in it, so damage to a single part of it can destabilize the entire SDS and cause a number of subsequent diseases.
Diseases of the musculoskeletal system are extremely diverse. They can be roughly divided into diseases of the skeletal system, joints and skeletal muscles.
Diseases of the skeletal system
Diseases of this group can be dystrophic, inflammatory, dysplastic and tumoral in nature. Dystrophic bone diseases (osteodystrophy) are divided into toxic (for example, Urovsky disease), nutritional (for example, rickets - see. Vitamin deficiencies), endocrine, nephrogenic (see. Kidney diseases). Among bone diseases dystrophic nature matters most parathyroid osteodystrophy. Inflammatory bone diseases are most often characterized by the development of purulent inflammation of the bone marrow (osteomyelitis), often bone tissue is affected by tuberculosis and syphilis (see. Infectious diseases). Dysplastic bone diseases are most common in children, but can also develop in adults. Among them, the most common fibrous bone dysplasia, osteopetrosis, Paget's disease. Against the background of dysplastic bone diseases, bone tumors(cm. Tumors).
Parathyroid osteodystrophy(Recklinghausen's disease, generalized osteodystrophy) is a disease caused by hyperfunction of the parathyroid glands and accompanied by generalized skeletal damage. The disease occurs mainly in women 40-50 years old, rarely in childhood.
Etiology. Parathyroid osteodystrophy is associated with primary hyperparathyroidism, which is caused by adenoma of the parathyroid glands or hyperplasia of their cells (cancer is very rare). Primary hyperparathyroidism should be distinguished from secondary hyperparathyroidism, which develops with chronic renal failure, multiple cancer metastases to the bones, etc. The importance of hyperfunction of the parathyroid glands in the development of bone pathology was first substantiated by A.V. Rusa-
kov (1924), who proposed for treatment bone pathology surgical removal of tumors of the parathyroid glands.
Pathogenesis. Increased synthesis of parathyroid hormone causes increased mobilization of phosphorus and calcium from the bones, which leads to hypercalcemia and progressive demineralization of the entire skeleton. Osteoclasts are activated in bone tissue, and foci of lacunar bone resorption appear. Along with this, diffuse fibroosteoclasia increases - bone tissue is replaced by fibrous connective tissue. These processes are most intensely expressed in the endosteal parts of the bones. In areas of intense restructuring, bone structures do not have time to mature and calcify; osteoid tissue, cysts, cavities filled with blood and hemosiderin are formed. Bone deformation and osteoporosis progress, and pathological fractures often occur. Formations appear in the bones that are indistinguishable from giant cell tumors (osteoblastoclastoma, according to A.V. Rusakov). In contrast to true tumors, these are reactive structures, which are giant cell granulomas in foci of organization of blood accumulations; they usually disappear after removal of the parathyroid tumor.
Hypercalcemia, which develops with parathyroid osteodystrophy, leads to the development of calcareous metastases, see. Violations mineral metabolism(mineral dystrophies). Nephrocalcinosis often develops, combined with nephrolithiasis and complicated by chronic pyelonephritis.
Pathological anatomy. In the parathyroid glands, adenoma is most often found, cell hyperplasia is less common, and cancer is even less common. The tumor may have an atypical localization - in the thickness thyroid gland, mediastinum, behind the trachea and esophagus.
Skeletal changes in parathyroid osteodystrophy depend on the stage and duration of the disease. IN initial stage illness and with low activity of parathyroid hormone, external changes in bones may be absent. In an advanced stage, deformation of bones is detected, especially those that are exposed to physical activity- limbs, spine, ribs. They become soft, porous, and can be easily cut with a knife. Bone deformation can be caused by multiple tumor-like formations, which have a variegated appearance when cut: yellowish areas of tissue alternate with dark red and brown ones, as well as cysts.
At in the bone tissue, foci of lacunar resorption are identified (Fig. 243), neoplasms of fibrous tissue, and sometimes osteoid beams. In the foci of tumor-like formations, giant cell granulomas, accumulations of erythrocytes and hemosiderin, and cysts are found.
Death In patients, it often occurs from cachexia or uremia due to shrinkage of the kidneys.
Rice. 243. Parathyroid osteodystrophy. Lacunar bone resorption (shown by arrows) and new formation of fibrous tissue (according to M. Eder and P. Gedik)
Osteomyelitis
Under osteomyelitis(from Greek osteon- bone, myelos- brain) understand inflammation of the bone marrow, spreading to the compact and spongy bone and periosteum. Osteomyelitis is divided into the nature of the current - on spicy And chronic, according to the mechanism of bone marrow infection - on primary hematogenous And secondary (a complication of injury, including a gunshot wound, during the transition of the inflammatory process from surrounding tissues). Highest value has primary hematogenous osteomyelitis.
Primary hematogenous osteomyelitis can be acute and chronic. Acute hematogenous osteomyelitis, usually develops in at a young age, 2-3 times more often in men. usually the outcome of an acute
Etiology. In the occurrence of osteomyelitis, the main role is played by pyogenic microorganisms: hemolytic staphylococcus(60-70%), streptococci (15-20%), coliform bacilli (10-15%), pneumococci, gonococci. Less commonly, fungi can be causative agents of osteomyelitis. The source of hematogenous spread of infection can be an inflammatory focus in any organ, but often primary focus cannot be detected. It is believed that such patients have transient bacteremia due to minor intestinal trauma, dental diseases, and upper respiratory tract infections.
Pathogenesis. The peculiarities of the blood supply to bone tissue contribute to the localization of infection in long tubular bones. Usually the purulent process begins from the bone marrow spaces of the metaphyses, where blood
the flow is slow. Subsequently, it tends to spread, causing extensive necrosis and spreading to the cortical bone, periosteum and surrounding tissues. Purulent inflammation spreads along the bone marrow canal, affecting more and more areas of the bone marrow. In children, especially newborns, due to the weak attachment of the periosteum and the peculiarities of the blood supply to the cartilage of the epiphyses, the purulent process often spreads to the joints, causing purulent arthritis.
Pathological anatomy. At acute hematogenous osteomyelitis the inflammation is phlegmonous (sometimes serous) in nature and involves the bone marrow, Haversian canals and periosteum; Foci of necrosis appear in the bone marrow and lamina compacta. Severe bone resorption near the epiphyseal cartilage can cause separation of the metaphysis from the epiphysis (epiphysiolysis), mobility and deformation of the periarticular zone appear. Around the foci of necrosis, tissue infiltration with neutrophils is determined, and blood clots are found in the vessels of the lamina compacta. Abscesses are often found under the periosteum, and phlegmonous inflammation is found in the adjacent soft tissues.
Chronic hematogenous osteomyelitis associated with chronic suppurative process, formation bone sequesters. Granulation tissue and a capsule are formed around the sequesters. Sometimes the sequestrum floats in a cavity filled with pus, from which fistulous tracts extend to the surface or cavities of the body, to the cavity of the joints. Along with this, bone formation is observed in the periosteum and medullary canal. Bones become thick and deformed. Endosteal bone growths (osteophytes) can lead to obliteration of the medullary canal, and the compact lamina thickens. At the same time, focal or diffuse irritation of the bone occurs due to its resorption. Foci of suppuration in soft tissues in the chronic course of hematogenous osteomyelitis usually scar.
Special shape chronic osteomyelitis is Brody's abscess. It is represented by a cavity filled with pus, with smooth walls, which are lined from the inside with granulations and surrounded by a fibrous capsule. In granulation tissue, many plasma cells and eosinophils are detected. No fistulas are formed, bone deformation is insignificant.
Complications. Bleeding from fistulas, spontaneous bone fractures, formation of false joints, pathological dislocations, development of sepsis; in chronic osteomyelitis, secondary amyloidosis is possible.
Fibrous dysplasia
Fibrous dysplasia(fibrous osteodysplasia, fibrous bone dysplasia, Lichtenstein-Braitsev disease) - a disease characterized by the replacement of bone tissue fibrous tissue, which leads to bone deformation.
Etiology and pathogenesis. The reasons for the development of fibrous dysplasia are not clear enough, and the role of heredity cannot be ruled out. Think that
The disease is based on a tumor-like process associated with improper development of osteogenic mesenchyme. The disease often begins in childhood, but can develop in young adulthood and old age. The disease predominates in females.
Classification. Depending on the distribution of the process, two forms of fibrous dysplasia are distinguished: monoosseous, in which only one bone is affected, and polyostotic, in which several bones are affected, mainly on one side of the body. The polyostotic form of fibrous dysplasia can be combined with melanosis of the skin and various endocrinopathies (Albright's syndrome). The monostotic form of fibrous dysplasia can develop at any age, the polyostotic form - in childhood, therefore, patients with this form of fibrous dysplasia have diffuse skeletal deformation and a predisposition to multiple fractures.
Pathological anatomy. In the monoosseous form of fibrous dysplasia, the ribs, long tubular bones, scapulae, and skull bones are most often affected (Fig. 244); with the polyostotic form - over 50% of the bones of the skeleton, usually on one side. The lesion may involve a small area or a significant part of the bone. In tubular bones it is localized mainly in the diaphysis, including the metaphysis. The affected bone at the beginning of the disease retains its shape and size. Subsequently, areas of “bloating”, bone deformation, elongation or
 shortening. Under the influence of static load, the femurs sometimes take on the shape of a shepherd's crook. When the bone is cut, clearly defined foci of a whitish color with reddish inclusions are identified. They are usually round or elongated, sometimes merging with each other; in places of “swelling” the cortical layer becomes thinner. The medullary canal is expanded or filled with newly formed tissue, in which lesions are identified bone density, cysts.
shortening. Under the influence of static load, the femurs sometimes take on the shape of a shepherd's crook. When the bone is cut, clearly defined foci of a whitish color with reddish inclusions are identified. They are usually round or elongated, sometimes merging with each other; in places of “swelling” the cortical layer becomes thinner. The medullary canal is expanded or filled with newly formed tissue, in which lesions are identified bone density, cysts.
At microscopic examination foci of fibrous dysplasia are represented by fibrous fibrous tissue, among which poorly calcified bone beams of a primitive structure and osteoid beams are identified (see Fig. 244). Fibrous tissue in some areas consists of chaotically located bundles of mature collagen fibers and spindle cells, in other areas - from developing (thin) collagen fibers and stellate cells. Sometimes myxomatous foci, cysts, accumulations of osteoclasts or xanthoma cells, and islands of cartilaginous tissue are found. Some features of the histological picture of fibrous dysplasia of the facial bones are noted: the dense component in the foci of dysplasia can be represented by cement-type tissue (cementicle-like formations).
Complications. Pathological bone fractures are the most common. In young children, often during their first attempts to walk, the femur is especially likely to break. Fractures upper limbs rare. Typically, fractures heal well, but bone deformation increases. In a number of observations, sarcoma develops against the background of fibrous dysplasia, often osteogenic.
Osteopetrosis
Osteopetrosis(marble disease, congenital osteosclerosis, Albers-Schönberg disease) is a rare hereditary disease in which there is generalized excessive bone formation, leading to thickening of the bones, narrowing and even complete disappearance of the medullary spaces. Therefore, osteopetrosis is characterized by a triad: increased bone density, fragility and anemia.
Etiology and pathogenesis. The etiology and pathogenesis of osteopetrosis have not been sufficiently studied. Undoubtedly, the participation of hereditary factors is associated with impaired development of bone and hematopoietic tissue. In this case, excessive formation of functionally inferior bone tissue occurs. It is believed that the processes of bone production prevail over its resorption, which is associated with the functional failure of osteoclasts. Increasing displacement of bone marrow by bone is associated with the development of anemia, thrombocytopenia, and the appearance of foci of extramarrow hematopoiesis in the liver, spleen, and lymph nodes, which leads to their enlargement.
Classification. There are two forms of osteopetrosis: early (autosomal recessive) and late (autosomal dominant). Early
form osteopetrosis manifests itself in early age, has a malignant course, often ending in death; late form proceeds more benignly.
Pathological anatomy. With osteopetrosis, the entire skeleton can be affected, but especially the tubular bones, bones of the base of the skull, pelvis, spine, and ribs. In the early form of osteopetrosis, the face has a characteristic appearance: it is wide, with widely spaced eyes, the root of the nose is depressed, the nostrils are deployed, and the lips are thick. With this form, hydrocephalus, increased hair growth, hemorrhagic diathesis, multiple lesions bones, whereas in the late form of osteopetrosis, bone damage is usually limited.
The outlines of the bones may remain normal, with only a flask-shaped expansion characteristic lower sections femurs. Bones become heavy and difficult to saw. On cuts in long bones the medullary canal is filled with bone tissue and is often not detected. In flat bones, the medullary spaces are also barely visible. In place of the spongy substance, dense, homogeneous bone tissue is found, reminiscent of polished marble (marble disease). Bone growth in the area of the holes and canals can lead to compression and atrophy of the nerves. This is what is associated with the most common optic nerve atrophy and blindness in osteopetrosis.
Microscopic picture extremely unique: pathological bone formation occurs throughout the entire bone, the mass of bone substance is sharply increased, the bone substance itself is randomly piled up in the internal parts of the bones (Fig. 245). Bone marrow
 Rice. 245. Osteopetrosis. Disorderly pile bone structures(according to A.V. Rusakov)
Rice. 245. Osteopetrosis. Disorderly pile bone structures(according to A.V. Rusakov)
the spaces are filled with randomly arranged layered bone conglomerates or lamellar bone with arcuate lines of adhesion; Along with this, beams of embryonic coarse fibrous bone are found. Single areas of ongoing bone formation are visible in the form of clusters of osteoblasts. Osteoclasts are rare, signs of bone resorption are insignificant. The architecture of the bone, due to the disordered formation of bone structures, loses its functional characteristics, which is obviously associated with bone fragility in osteopetrosis. In zones of enchondral ossification, cartilage resorption is practically absent. On the basis of the cartilage, peculiar rounded islands of bone beams are formed, which gradually turn into wide beams.
Complications. Bone fractures often occur, especially the femur. In places of fractures, purulent osteomyelitis often develops, which is sometimes a source of sepsis.
Causes of death. Patients with osteopetrosis often die in early childhood from anemia, pneumonia, and sepsis.
Paget's disease
Paget's disease(deforming ostosis, deforming osteodystrophy) - a disease characterized by increased pathological restructuring of bone tissue, a continuous change in the processes of resorption and new formation of bone substance; in this case, the bone tissue acquires a peculiar mosaic structure. The disease was described in 1877 by the English physician Paget, who considered it inflammatory and called it deforming osteitis.
Later, the inflammatory nature of the disease was rejected, and the disease was classified as a dystrophic disease. A.V. Rusakov (1959) was the first to prove the dysplastic nature of Paget's disease.
The disease is observed more often in men over 40 years of age, progresses slowly, and usually becomes noticeable only in old age. It is believed that asymptomatic forms of the disease occur with a frequency of 0.1-3% in different populations. The process is localized in long tubular bones, skull bones (especially facial), pelvic bones, vertebrae. The lesion may involve only one bone (monostotic form) or several often paired or regional bones (polyostotic form), but it is never generalized, which distinguishes Paget's disease from parathyroid osteodystrophy.
Etiology. The reasons for the development of the disease are not known. Violation of phosphorus-calcium metabolism, viral infection How possible reason Paget's disease is excluded, but the familial nature of the disease is noted. The dysplastic nature of bone lesions in Paget's disease is evidenced by the non-functional nature of bone restructuring and the frequent development of sarcoma against this background.
Patho- and morphogenesis. The processes of bone tissue restructuring in Paget's disease occur continuously, and there is no connection with the functional load. Depending on the relationship between the process of osteolysis and osteogenesis, 3 phases of the disease are distinguished: initial (osteolytic), active (a combination of osteolysis and osteogenesis) and inactive (osteosclerotic). IN initial phase Bone resorption processes predominate with the participation of osteoclasts, and therefore deep lacunae are formed in the bone tissue. IN active phase deforming ostosis, along with osteolysis, new bone formation is also expressed; osteoblasts appear, lacunae are filled with newly formed bone substance. Wide, clear bonding lines appear where the old and new bone meet. Due to the constant repetition and change of the processes of osteolysis and osteogenesis, bone beams are built from small fragments that form a characteristic mosaic. For inactive phase characterized by the predominance of the process of osteosclerosis.
Pathological anatomy. Bone changes in Paget's disease are quite characteristic. Long tubular bones especially the femur and tibia, are curved, sometimes spiral-shaped, which is explained by the growth (elongation) of the bone during its restructuring. At the same time, the length of a healthy paired bone does not change. The surface of the affected bone is rough, cuts reveal a narrow medullary canal, sometimes it is completely obliterated and filled with randomly alternating beams. When the periosteum is removed, small numerous openings of the vascular canals are usually visible on the surface of the cortical layer (normally they are almost invisible). This is due to the fact that bone restructuring is accompanied by intense resorption of the bone walls of the vascular canals and a sharp dilation of blood vessels. When cut, the cortical layer of the bone loses its compact structure and becomes spongy. However, this is only an external resemblance to spongy tissue, since the restructuring in Paget's disease is afunctional in nature.
In case of defeat skull bones the process usually involves only the bones of the skull. In the bones of the roof of the skull there is no division into the inner, outer plate and middle spongy layer; the entire bone mass has an unevenly spongy structure with areas of rarefaction and compaction. If the bones of the facial skull are also changed, then the face becomes sharply disfigured. The thickness of the bones when cut can reach 5 cm, and the thickening of the bone can be either uniform or uneven. Despite the increased volume, the bones are very light, which is due to the decrease in lime in them and the presence of a large number of pores.
IN spine the process involves one or more vertebrae in any of its parts, but the whole thing is never affected spinal column. The vertebrae increase in volume or, on the contrary, flatten, which depends on the stage of the disease. Foci of osteoporosis are found on the cuts and
osteosclerosis. Pelvic bones may also be involved in a pathological process that involves one or all bones.
Microscopic examination convinces us that the structural features of bone tissue in Paget's disease reflect its pathological restructuring. The mosaic structure of bone structures characteristic of Paget's disease is associated with the continuous change in the processes of resorption and construction of bone substance (Fig. 246). Small fragments of bone structures with uneven contours and wide, clearly defined basophilic adhesion lines are identified. The areas of bone fragments of the mosaic are usually well calcified, their structure is disordered, fine-fibrous or lamellar. Sometimes osteoid structures are found. In the deep lacunae of bone structures, a large number of osteoclasts and axillary resorption cavities are found. Along with this, signs of new bone formation are noted: expanded bone spaces are filled with soft fibrous tissue. The processes of bone restructuring also involve the vascular bed; usually the caliber of the feeding arteries is sharply increased, they acquire a sharp tortuosity.
Complications. Hemodynamic disorders, pathological fractures, development of osteogenic sarcoma. Hemodynamic disorders, associated with vasodilation in the affected bone tissue, in the skin over the lesions, can cause heart failure in patients with bone lesions of more than a third of the skeleton. Pathological fractures usually develop in active phase diseases. Osteogenic sarcoma develops in 1-10% of patients with deforming ostosis. Sarcoma is most often localized in the femur, tibia, pelvic bones, zygomatic bone, and scapula; primary multiple sarcomas have been described.
 Rice. 246. Paget's disease. Mosaic bone structure (according to T.P. Vinogradova)
Rice. 246. Paget's disease. Mosaic bone structure (according to T.P. Vinogradova)
Joint diseases
Joint diseases may be associated with dystrophic (“degenerative”) processes structural elements joints (arthrosis) or their inflammation (arthritis). The synovium of the joint and cartilage can be a source of tumor (see. Tumors). Arthritis may be associated with infections(infectious arthritis), be a manifestation rheumatic diseases(cm. Systemic diseases connective tissue), metabolic disorders(For example, gouty arthritis, cm. Disorders of nucleoprotein metabolism) or other diseases (for example, psoriatic arthritis).
The most important among arthrosis is osteoarthritis, among arthritis - rheumatoid arthritis.
Osteoarthritis
Osteoarthritis- one of the most common joint diseases of a dystrophic (“degenerative”) nature. Elderly women are more often affected. Osteoarthritis is divided into primary (idiopathic) and secondary (for others, such as endocrine diseases). As you can see, osteoarthritis is a collective concept that unites a large number of diseases. However, there are no significant differences between primary and secondary osteoarthritis. The joints of the lower extremities are most often affected - the hip, knee, ankle, and somewhat less frequently - the large joints of the upper extremities. Usually the process simultaneously or sequentially involves several joints.
Etiology and pathogenesis. For the development of osteoarthritis, predisposing factors are important - hereditary and acquired. Among hereditary factors special meaning give a genetically determined metabolic disorder in articular cartilage, especially a disorder of the catabolism of its matrix. From acquired Mechanical injury plays a leading role.
Classification. Based on clinical and morphological manifestations, 3 stages of osteoarthritis are distinguished. In stage I, pain in the joints is noted during exercise, and x-rays reveal a narrowing of the joint space and osteophytes. In stage II, pain in the joints becomes constant, narrowing of the joint space and the development of osteophytes with x-ray examination more pronounced. In stage III, along with constant joint pain functional joint insufficiency is noted due to the development of subchondral sclerosis.
Pathological anatomy. Macroscopic changes in osteoarthritis depend on the stage of its development. In the early (I) stage, roughness and tissue disintegration appear along the edges of the articular cartilage. Later (stage II) on the articular surface of the cartilage they find patterns And lumps, bone growths are formed - osteophytes. In the advanced (III) stage of the disease, articular cartilage disappears on the bones of the joints
Dents form and the joints themselves become deformed. The intra-articular ligaments are thickened and loosened; the folds of the articular capsule are thickened, with elongated papillae. The amount of synovial fluid is sharply reduced.
Microscopic characteristics stages of osteoarthritis have been well studied (Kopyeva T.N., 1988). In stage I, articular cartilage retains its structure; in its superficial and intermediate zones, the content of glycosaminoglycans decreases. In stage II, shallow lesions appear in the superficial zone of the cartilage, along the edge of which chondrocytes accumulate, and the content of glycosaminoglycans in all zones of the cartilage decreases. If there are no abnormalities in the superficial zone of cartilage, then in the superficial and intermediate zones the number of “empty lacunae”, chondrocytes with pyknotic nuclei, increases. The subchondral part of the bone is also involved in the process. In stage III of osteoarthritis, the superficial zone and part of the intermediate zone of the cartilage die, deep lesions are found, reaching the middle of the intermediate zone; in the deep zone, the content of glycosaminoglycans is sharply reduced, the number of chondrocytes with pyknotic nuclei is increased. The damage to the subchondral part of the bone intensifies. At all stages of osteoarthritis in synovium joints are found synovitis varying degrees of severity, lymphomacrophage infiltrate and moderate proliferation of fibroblasts are found in the synovium; as a result of synovitis, sclerosis of the stroma and vascular walls develops.
Rheumatoid arthritis
Rheumatoid arthritis- one of the most bright manifestations rheumatic diseases (see Systemic connective tissue diseases).
Skeletal muscle diseases
Among skeletal muscle diseases, the most common are diseases of striated muscle dystrophic (myopathies) and inflammatory (myositis) character. Muscles can be the source of a number of tumors (see. Tumors). Of particular interest among myopathy are progressive muscular dystrophy (progressive myopathy) and myopathy in myasthenia gravis.
Progressive muscular dystrophy(progressive myopathy) includes various primary hereditary chronic diseases of the striated muscles (they are called primary because the lesion spinal cord and peripheral nerves are absent). The diseases are characterized by increasing, usually symmetrical, muscle atrophy, accompanied by progressive muscle weakness, up to complete immobility.
Etiology and pathogenesis little studied. The significance of anomalies in structural proteins, sarcoplasmic reticulum, innervation, and enzymatic activity of muscle cells is discussed. Characterized by an increase in the activity of muscle enzymes in the blood serum, corresponding electrophysiological disorders in damaged muscles, and creatinuria.
Classification. Depending on the type of inheritance, age, gender of patients, localization of the process and course of the disease, there are 3 main forms of progressive muscular dystrophy: Duchenne, Erb and Leiden. The morphological characteristics of these forms of muscular dystrophy are similar.
Duchenne muscular dystrophy(early form) with a recessive type of inheritance associated with the X chromosome, usually appears at the age of 3-5 years, more often in boys. First, the muscles of the pelvic girdle, thighs and legs are affected, then the shoulder girdle and torso. Erb's muscular dystrophy(adolescent form) has an autosomal dominant type of inheritance and develops from puberty. The muscles of the chest and shoulder girdle, sometimes the face, are mainly affected (myopathic face - smooth forehead, insufficient eye closure, thick lips). Possible atrophy back muscles, pelvic girdle, proximal limbs. Muscular dystrophy Leiden with an autosomal recessive type of inheritance begins in childhood or during puberty and proceeds more quickly compared to the juvenile form (Erba), but more favorably than the early form (Duchenne). The process, starting with the muscles of the pelvic girdle and hips, gradually involves the muscles of the torso and limbs.
Pathological anatomy. Usually the muscles are atrophic, thinned, depleted of myoglobin, so when cut they resemble fish meat. However, muscle volume can be increased due to the vacant growth of fatty tissue and connective tissue, which is especially typical for Duchenne muscular dystrophy (pseudohypertrophic muscular dystrophy).
At microscopic examination muscle fibers have different sizes: along with atrophic ones, there are sharply enlarged ones; the nuclei are usually located in the center of the fibers. Dystrophic changes in muscle fibers (accumulation of lipids, decrease in glycogen content, disappearance of cross-striations), their necrosis and phagocytosis are pronounced. Signs of regeneration are determined in individual muscle fibers. Fat cells accumulate between damaged muscle fibers. At severe course The disease reveals only single atrophic muscle fibers among extensive growths of adipose and connective tissue.
Ultrastructural changes in muscle fibers have been studied in more detail in Duchenne muscular dystrophy (Fig. 247). At the onset of the disease, expansion of the sarcoplasmic reticulum, foci
 Rice. 247. Duchenne muscular dystrophy. Necrosis of muscle fiber with destruction of myofibrils. x 12,000
Rice. 247. Duchenne muscular dystrophy. Necrosis of muscle fiber with destruction of myofibrils. x 12,000
destruction of myofibrils, expansion of interfibrillar spaces in which the amount of glycogen increases, movement of nuclei to the center of the fiber. In the late stage of the disease, myofibrils undergo fragmentation and disorganization, mitochondria are swollen, the T-system is expanded; in muscle fibers the number of lipid inclusions and glycogen increases, and autophagolysosomes appear. At the end of the disease, the muscle fibers become denser, surrounded by a hyaline-like substance, and macrophages and fat cells appear around the necrotic muscle fibers.
Death In patients with severe progressive muscular dystrophy, it usually occurs from pulmonary infections.
Myasthenia gravis
Myasthenia gravis(from Greek myos- muscle, asthenia- weakness) - chronic illness, the main symptom of which is weakness and pathological fatigue of the striated muscles. Normal muscle contraction after vigorous activity decreases in strength and volume and may stop completely. After rest, muscle function is restored. In an advanced stage of the disease, the rest time increases, creating the impression of muscle paralysis. With myasthenia gravis, any muscles of the body can suffer, but more often the muscles of the eyes (ptosis develops in 80% of cases), chewing, speech, and swallowing. In the extremities, the proximal muscles of the shoulder and thigh are most often affected. The respiratory muscles may also be affected.
The disease occurs at any age (peak incidence is 20 years), 3 times more often in women compared to men.
Etiology and pathogenesis. Etiology unknown. There is a correlation between anomalies thymus gland and myasthenia. Thymectomy often gives positive effect. The development of the disease is associated with a decrease of up to 90% in the number of acetylcholine receptors per unit of muscle plate, which is caused by autoimmune reactions. Antibodies to acetylcholine receptors were extracted from the thymus gland, they were found in the blood serum (in 85-90% of patients), using the immunoperoxidase method, IgG and C 3 were constantly detected in postsynaptic membranes. It is possible that not only antibodies, but also effector immune cells are involved in the blockade of acetylcholine receptors.
Pathological anatomy. In the thymus gland of patients with myasthenia gravis, follicular hyperplasia or thymoma is often found. Skeletal muscles are usually slightly changed or are in a state of dystrophy, sometimes their atrophy and necrosis, focal accumulations of lymphocytes among muscle cells are noted. Using immune electron microscopy, it is possible to detect IgG and C 3 in postsynaptic membranes. In the liver thyroid gland, adrenal glands and other organs find lymphoid infiltrates.
The musculoskeletal system performs the musculoskeletal function. It consists of a skeleton (Fig. 1), the bones of which serve as levers, and striated muscles attached to the bones, which act as a power unit.
The skeleton consists of bones and their joints. It performs the functions of support, movement and protection. The supporting function is manifested in the fact that the skeleton supports other organs, gives the body a constant shape and allows it to take certain positions. Skeletal bones, within certain limits, provide protection for internal vital organs from external harsh physical influences. So, the brain is in cranium, and the dorsal one - in spinal canal, the bones of the chest protect the heart, lungs and other organs located in it, and the bones of the pelvis protect the organs of the genitourinary system.
According to their shape, all bones are divided into long (tubular bones of the limbs), short (vertebrae, heel bone) and flat (scapula, ribs, pelvic bones). All bones are covered with periosteum, which is a connective tissue plate tightly fused with the bone. From her nerve fibers and vessels penetrate the bone and provide metabolic processes. Special cells of the periosteum - osteoblasts - are involved in the formation of bone tissue both during its growth and during healing after fractures.
Rice. 1. Human skeleton:
1 - skull; 2 - spinal column; 3 - collarbone; 4 - rib; 5 - sternum; 6 - humerus; 7 - radius; 8 - elbow bone; 9 - carpal bones; 10 - metacarpus bones; 11 - phalanges of the fingers; 12 - pelvic bones; 13 - femur; 14 - patella; 15 - tibia; 16 - fibula; 17 - tarsal bones; 18 - metatarsal bones
The chemical composition of bones is represented by water, fat, osein - an organic substance that provides elasticity, and inorganic salts that give them hardness. With age, the amount of organic matter in a person decreases, and the amount of inorganic salts increases - bones lose elasticity and become fragile.
The bones of the skeleton, connecting with each other, form a skeleton, and depending on the functional characteristics of the joints they can be fixed, sedentary and mobile. In motionless ones, there is no or very slight movement. Such joints are formed with the help of fibrous connective tissue (bones of the wrist, tarsus, vertebral arches, etc.) or with the help of cartilage (bones of the calvarium, sacral vertebrae). Sedentary joints - semi-joints (pubic, sacrococcygeal and some other joints) are distinguished by the presence of the rudiments of an articular cavity. The movable joints of bones are called joints. In them, the articulating surfaces of the bones are covered with cartilage and isolated from the surrounding tissues by the articular capsule, which, attached at the edges articular surfaces, forms an articular cavity. The articular cavity contains a small amount of viscous liquid that reduces friction of articular surfaces. Depending on the function, the joints come in different shapes: spherical, allowing movement in three planes (shoulder, hip); ellipsoidal, providing movement in two planes (connection of the skull with the first vertebra); block-shaped, allowing movements only in one plane (knee, elbow); flat, allowing displacement (articular processes of the vertebrae), etc.
Skeletal muscles provide all movements associated with walking, eating and labor processes. A person has about 600 pairs of them, and they make up almost 40% of his body weight. Muscles attach to bones directly or through tendons. They are thrown through 1-2 or more joints and, when contracted, cause the bones to move: flexion, extension, adduction, abduction or rotation. Skeletal muscles are conventionally divided by function into synergists, which produce movement in one direction, and antagonists, which act in the opposite direction. Almost every movement is a complex act involving many muscles. The magnitude of the efforts and the strict sequence of their contractions and relaxations are coordinated by the central nervous system (CNS).
Skeletal muscles, thanks to impulses arriving through the motor nerves from the central nervous system, are in constant tone - a state of some tension. This ensures a stable body position. Intensity increases sharply in the working muscle metabolic processes and the amount of oxygen supplied becomes insufficient. An accumulation of under-oxidized metabolic products occurs, and fatigue develops in the muscle, which results in a decrease in the strength of contractions. To increase muscle performance, training is crucial.




