Types and signs of fractures. Signs of dislocations in the joints. Rules and methods of providing first aid for bone fractures and dislocations. Rules for applying splints. Application of splints and immobilization of joints for certain types of fractures and dislocations using report cards
The adult skeleton contains more than two hundred bones (infants have more, but then some bones fuse together). And each of the bones can be broken. Can you imagine how many types of fractures and first aid methods medical students need to learn? Of course, the scope of one article does not allow us to consider absolutely all types of bone injuries. Here you will receive information about the main types of fractures, their signs and first aid to the victim before the doctor arrives.
Signs of open and closed fractures
Fracture- this is a complete or partial violation of the integrity of the bone as a result of mechanical damage.
Fractures can be open or closed, the differences between them are as follows:
- with closed injuries there is no damage to the skin, bone fragments are located in the thickness of the soft tissues;
- with open injuries, bone fragments break through the surrounding soft tissue and skin.
With closed fractures, severe hemorrhage quickly appears at the site of injury. The intensity of pain can range from insignificant to unbearable; it intensifies not only from movement of the injured limb, but also from changes in body position. The limb itself either lengthens or shortens, and begins to bend in completely inappropriate places. When palpating the area, a crunching sound of bone fragments is detected. The affected limb completely loses its function.
In case of open fractures, the injury is accompanied by external bleeding, severe - in case of damage large vessels, minor - when small ones rupture; bone fragments are visible in the open wound.
Having identified the symptoms of a fracture, first aid should be provided immediately.
Clavicle fractures: types, symptoms and first aid
The collarbone may break in the middle or at the ends.
There are two types of clavicle fractures:
- straight - occur when falling on outstretched arm;
- indirect - occur when the shoulder joints are compressed from the sides.
With a central fracture, the fragment moves upward and backward, and with a peripheral fracture, downward and anteriorly. The bone is deformed and moves in different directions. The site of injury swells, and when palpated, a crunching sound of bone fragments is detected. The arm, together with the shoulder joint, is turned inward, lowered down and shifted forward. Another symptom of a clavicle fracture is flattening of the supraclavicular fossa.
Before providing assistance for a fractured collarbone, the victim is given an anesthetic, for example 2 ml of ketorol. The effect of the drug can be enhanced if suprastin, diphenhydramine or any other antihistamine is simultaneously administered. A good analgesic effect is obtained by injecting the fracture site with a 1-2% solution of novocaine (no more than 10-15 ml). Then, when providing first aid for a fractured collarbone, the injured limb is immobilized by hanging the arm on a scarf or bandaging it to the body.
The victim is transported to the emergency room in a sitting position.
Types and signs of shoulder fractures, first aid
 There are three types of shoulder fracture: upper third, middle third and lower third of the bone.
There are three types of shoulder fracture: upper third, middle third and lower third of the bone.
When the upper third of the bone (near the shoulder joint) is fractured, the victim complains of severe pain in the shoulder joint, which intensifies with the slightest movement and touch. The joint itself is swollen. To reduce pain, a person bends his arm at the elbow joint and presses it to his body, supporting him with his healthy arm. Additional feature In case of a fracture, there may be a crunching of the fragments, which is sometimes felt when palpating the joint area.
If the victim seeks help late (more than a day after the injury), a bruise appears in the area of the elbow joint or even on the forearm.
Fractures in the middle third may damage the nerve running along the shoulder. In this case, the victim, in addition to the classic signs of a fracture (such as shortening and deformation of the shoulder, pathological bone mobility, clearly noticeable crunching of fragments), has signs of nerve damage: the hand hangs passively, it can only be straightened passively, active movements are impossible. Another sign of a shoulder fracture in the middle third is the inability to abduct the thumb.
In case of a fracture in the lower third of the bone, the protruding olecranon process is clearly contoured, above which the area of retraction is determined. The elbow joint swells and becomes sharply painful. At the site of injury, crunching of fragments is detected.
Before providing first aid for a fractured shoulder in the upper third, 2 ml of a 50% analgin solution is administered for pain relief (the effect of the drug can be enhanced if suprastin, diphenhydramine or any other antihistamine is simultaneously administered). The arm is suspended on a scarf; in case of severe pain, it is fixed to the body with a bandage.
If the middle part of the shoulder is fractured, the victim’s arm is fixed with a transport splint (instead, slats, straight sticks and tree branches, reinforcement, etc. can be used).
The splint is applied from the healthy shoulder blade to the base of the fingers. The arm is bent at a right angle at the elbow joint. For pain relief, 2 ml of a 50% analgin solution or 5 ml of baralgin solution are administered.
First aid for a fracture of the shoulder in the lower third consists of fixing the arm after anesthesia with a transport splint, bending the elbow joint at an angle of 90-100°.
Types of forearm fractures, symptoms and first aid
 There are many types of forearm fractures. When the olecranon is fractured, swelling and smoothness of the posterior surface of the joint occur; the person trying to keep the arm straight, pressing it with the healthy arm to the body; Active flexion at the elbow joint is possible, but extension is not.
There are many types of forearm fractures. When the olecranon is fractured, swelling and smoothness of the posterior surface of the joint occur; the person trying to keep the arm straight, pressing it with the healthy arm to the body; Active flexion at the elbow joint is possible, but extension is not.
When the coronoid process is fractured, swelling appears, maximum flexion is limited, and other movements are not impaired. A symptom of such a fracture of the forearm is the smoothness of the contours of the ulnar fossa.
A fracture of the upper radius occurs as a result of a fall on an outstretched arm. The victim cannot fully straighten his arm; sharp pain appears when trying to turn the forearm outward.
With a fracture of the ulna, active flexion and extension of the elbow joint are possible, other movements are carried out in a limited volume.
With a fracture of the radius, active movements are almost impossible due to severe pain.
A fracture of both bones is also possible. It usually occurs as a result of a direct blow to the forearm, the forearm and hand being pulled into moving parts of machines, or during a car accident. In this case, the forearm is noticeably deformed (while with a fracture of one bone, the deformation is not so pronounced), the bones are abnormally mobile, and when you feel the injured limb, a distinct crunching of the fragments is felt.
After administering an anesthetic (2 ml of 50% analgin solution, 2 ml of ketorol, 5 ml of baralgin), a transport splint is applied to the injured limb from the lower third of the shoulder to the base of the hand, bending the arm at the elbow joint at an angle of 90-100°. To reduce swelling, when providing first aid for a forearm fracture, cold is used.
Fractures of the hand: types, signs and first aid
 There are three main types of hand fractures:
There are three main types of hand fractures:
- fracture of the carpal bones;
- fracture of the metacarpal bones (I metacarpal and II-V metacarpal bones);
- fracture of the phalanges (main, middle and nail).
The main signs of hand fractures are acute pain, deformation (in case of displaced fractures) of the hand (or wrist), swelling, and crunching. When the nail phalanges are fractured, hemorrhages appear under the nails.
First aid for a broken hand consists of anesthetizing and immobilizing the damaged area. The victim is given a small ball (a bottle, a roller made from scrap materials) into the sore hand, and the fingers are bandaged to it in a half-bent state. Then the hand is suspended on a scarf.
Types and symptoms of hip fractures, assistance
 Hip fractures can occur in several places. Fractures that pass through the attachment of the femur to the pelvis occur when falling on one side. This type of hip fracture is characterized by very severe pain in the hip joint area, the limb is rotated outward so that the outer edge of the foot becomes parallel to the surface of the bed. At the site of injury, swelling quickly develops and hemorrhage appears. At the slightest attempt to lift the leg, very severe pain occurs. Shortening of the leg is not typical for this type of fracture. An additional sign of a fracture is sharp pain in the hip joint when the heel is tapped.
Hip fractures can occur in several places. Fractures that pass through the attachment of the femur to the pelvis occur when falling on one side. This type of hip fracture is characterized by very severe pain in the hip joint area, the limb is rotated outward so that the outer edge of the foot becomes parallel to the surface of the bed. At the site of injury, swelling quickly develops and hemorrhage appears. At the slightest attempt to lift the leg, very severe pain occurs. Shortening of the leg is not typical for this type of fracture. An additional sign of a fracture is sharp pain in the hip joint when the heel is tapped.
With a fracture of the femoral neck, the pain is much less than in the previous case, but the victim cannot lift the leg on his own, while the doctor lifts it, causing virtually no pain. This symptom of a hip fracture is called a “stuck heel.” Tapping the heel causes slight pain.
A fracture of the femur closer to the knee joint is possible with a direct impact, with a fall on a bent knee, or with a fall on straight legs. The injury is characterized by severe pain in the area knee joint. The joint itself is enlarged and deformed due to hemorrhage and displacement of bone fragments. Any attempt by active or passive movements is accompanied by increased pain and often causes crunching of the fragments.
After administering 2 ml of a 50% analgin solution to relieve pain, a splint is applied to the injured limb. To help with a hip fracture, the ankles are wrapped in soft material (cotton wool), two splints are placed on the leg - one on the inside, the other on the outside, covering not only the leg, but also the torso; the splints are bandaged, from above - directly to the chest.
Fractures of the lower leg bones: types, signs, first aid
 There are two types of tibia fractures: More often there is a fracture of both bones of the leg, less often - only one (tibia or fibula). The mechanism of injury is both direct (a strong blow to the shin, heavy objects falling on the leg) and indirect (sharp rotation of the shin with a fixed foot).
There are two types of tibia fractures: More often there is a fracture of both bones of the leg, less often - only one (tibia or fibula). The mechanism of injury is both direct (a strong blow to the shin, heavy objects falling on the leg) and indirect (sharp rotation of the shin with a fixed foot).
Fractures accompanied by displacement of bone fragments are quite easy to diagnose. With them, deformation and reduction in bone length are clearly visible. The site of injury is sharply painful, swollen, and hemorrhage quickly appears. When palpating the fracture, a crunching sound of the fragments is detected. The victim's attempts to lift his leg on his own end in failure.
Fractures of one bone are much more difficult to diagnose. In this case, the shape of the lower leg remains virtually unchanged, and the victim freely raises his leg. In this case, palpating the area of injury helps. At the site of the fracture, a sign of a tibia fracture is noted, such as local pain, which intensifies with passive and active movements of the foot, and tapping on the heel. In some cases, hemorrhage occurs here.
For pain relief, 2 ml of a 50% analgin solution is injected. Then, when providing first aid for a fractured leg, the victim is given a splint from the upper third of the thigh to the end of the toes.
Ankle and foot injuries, emergency care
 An ankle sprain is characterized by a rapid increase in swelling in this area due to hemorrhage and severe pain when attempting to move the joint. Sometimes the injury is complicated by a fracture of one of the bones of the dorsum of the foot. In this case, when palpating its base, acute pain occurs.
An ankle sprain is characterized by a rapid increase in swelling in this area due to hemorrhage and severe pain when attempting to move the joint. Sometimes the injury is complicated by a fracture of one of the bones of the dorsum of the foot. In this case, when palpating its base, acute pain occurs.
A fracture of the lateral malleolus also causes pain and swelling, but the area of greatest pain is located directly in the ankle area.
A fracture of both ankles with a subluxation of the foot is a very serious injury. The joint is very swollen, the foot is displaced to the side. Any movement, both passive and active, causes sharp pain, and in some cases, patients feel the crunching of fragments.
A calcaneal fracture is characterized by an increase in the volume of the heel and its displacement outward. Often there is a flattening of the arch of the foot. Pain occurs when trying to lean on the sore leg, when feeling the heel, and also when moving the ankle joint.
Emergency care for injuries to the ankle and foot involves applying a splint from the knee joint to the toes. Pain relief is carried out using 2 ml of a 50% analgin solution intramuscularly.
Signs of a pelvic fracture and how to provide first aid
Similar injuries occur when the pelvis is compressed, when falling from a height and when there is a strong blow to this area (when hit by a car). A single, isolated fracture of one of the bones, uncomplicated, most often passes without any serious consequences for the body, which cannot be said about multiple fractures of the pelvic bones. Such an injury often leads to severe internal bleeding, and the urinary tract is often damaged ( bladder, urethra). In most cases, this causes severe traumatic shock.
A sign of a fracture of the pelvic bones is severe pain at the site of injury, which intensifies even more when palpating the pubic area and ridges iliac bones. Over time, hemorrhage may appear in the area of the external genitalia. A characteristic sign of a fracture is the “stuck heel” symptom that appears on the injured side. In this case, the victim is unable to lift his heel off the bed.
Before assistance is provided for a fracture of the pelvic bones, the victim is placed on a rigid stretcher on his back. The knees are spread apart and a cushion is placed under them (the “frog” position). No splint required. If the stretcher is soft, then the victim is transported on his stomach. It is necessary to administer painkillers (analgin, baralgin).
Types of rib fractures, symptoms and first aid
 There are two types of hip fractures: isolated and multiple rib fractures. The causes of injury are most often a strong blow to the chest, a fall, etc. The older the person, the greater the likelihood of a fracture due to injury chest, because with age it becomes less and less elastic.
There are two types of hip fractures: isolated and multiple rib fractures. The causes of injury are most often a strong blow to the chest, a fall, etc. The older the person, the greater the likelihood of a fracture due to injury chest, because with age it becomes less and less elastic.
A sharp pain immediately occurs at the fracture site, which intensifies with breathing movements. Another symptom of a rib fracture is a decrease in the mobility of the chest on the side of the injury. When palpating the chest, it is possible to determine the place of greatest pain and feel the crunching of fragments. The victim breathes frequently and shallowly and tries to move as little as possible.
With multiple fractures of the ribs, when one or more bones are damaged in two places, during inhalation the area limited by the fractures sinks, and during exhalation, on the contrary, bulges, no matter how paradoxical it may sound. This condition very quickly leads to impaired respiratory function, and subsequently blood circulation.
Providing first aid for rib fractures begins with mandatory anesthesia with analgin solution (2 ml of a 50% solution). Then the victim’s chest is tightly bandaged (with a wide bandage, towel, sheet, etc.) and taken to the trauma center.
Spinal fracture: types, symptoms and how to provide first aid
 There are two main types of spinal fractures: injuries to the cervical vertebrae and injuries to the thoracic and lumbar regions.
There are two main types of spinal fractures: injuries to the cervical vertebrae and injuries to the thoracic and lumbar regions.
Damage to the cervical vertebrae occurs when the neck is sharply flexed or hyperextended. They are observed when falling on the head, in divers, in car injuries, especially in cases where the seats in the car are not equipped with head restraints. Some victims are complicated by spinal cord damage varying degrees gravity.
The injury manifests itself primarily as severe pain in the neck. To reduce it at least a little, a person supports his head with his hands and avoids turning and bending. If the integrity of the spinal cord is damaged, complete paralysis of the arms and legs occurs. The main symptom of this type of spinal fracture is the impossibility of active movements and loss of all types of sensitivity. In addition, acute urinary retention develops.
Injuries to the thoracic and lumbar spine most often occur when falling on the back, less often from an impact, falling from a height, or excessive bending. A sign of a fracture is pain in the corresponding area, which intensifies when palpating the injury site. The protruding process of the damaged vertebra is often clearly visible.
When providing first aid, if there is even the slightest suspicion of a spinal fracture, under no circumstances should you turn over or carry a person in the usual way as it can cause vertebral misalignment and damage to the spinal cord. Before providing first aid for a spinal fracture, in order to avoid such a complication, the victim must be shifted so that the head and neck remain in the same plane with the torso. First, he is turned over on his back. To do this, you need at least three people: one holds the patient’s head and neck, the second holds the torso, and the third holds the legs. The rotation is performed synchronously. After this, it is necessary to secure the victim’s arms and legs. The arms are placed on the chest and tied at the wrists, the legs are extended, the knees and ankles are tied.
To transport a person with a spinal fracture, a solid stretcher or a wooden shield is needed (from improvised means, you can use boards, cabinet doors, sheets of plywood, tin, plastic, flat slate, etc.). When providing first aid for a spinal fracture, a cushion (made from clothes, towels, etc.) is placed in advance at the location of the lower back. The three of them also lift the victim, synchronously. At this moment, the fourth person moves the stretcher under the patient, after which he is lowered in the same synchronized manner. It is strictly forbidden to seat a sick person! Before transportation, you must also secure the head with a roller or rubber circle.
This article has been read 7,664 times.
Remember as a child: “Don’t run! Watch your step! You’ll fall and break something!”? And then there were those “heroes” who, despite all the warnings, still managed to get away with it, and then proudly came to school with a cast, enthusiastically telling and desperately fibbing, of course, how everything really happened.
However, if we put aside the peculiar “heroism” of teenagers, we understand that there is nothing funny or funny about injuries of this kind, and that they are quite fragile, and a fracture of, say, a limb can change our usual way of life for a long time.
Realizing the seriousness of the consequences, sometimes even having fallen slightly, we listen to ourselves with fear, trying to dissuade ourselves and denying, one by one, all the signs of a fracture.
So, first of all, it should be noted that a fracture is a violation of the integrity of the bone, which, as a rule, occurs as a result of various types of injuries.
In turn, the influence of a traumatic factor can be of two types: direct (impact) and indirect (high axial load on the bone).
Most often, the severity of the injury directly depends on the impact.
Let us recall, by the way, that all bones can be divided into spongy and tubular. They have different structures, and therefore differ from each other in their properties. For example, (the lower and upper limbs of a person) are capable of withstanding significantly greater loads, but at the same time they are less elastic compared to spongy limbs.
Types and signs of bone fracture:
There are several types of fractures, among them, for example, transverse and spiral ones are often found, but multidirectional fractures resulting from splintered injuries are considered the most dangerous.
The latter type is most often the result of a fall from a height or traffic accidents.
Some fractures occur without displacement of the axis, but sometimes, in more severe cases, several lines of fractures appear, and the fragments are significantly displaced. The latter type leads to deformation of a part of the body.
Often the sharp edge of a bone fragment injures nearby vessels, resulting in fractures that are further complicated by heavy bleeding. In some cases, fragments can also injure nerve trunks in case of spinal cord fractures, the brain in case of severe craniocerebral injuries, and injuries to the lungs and pleura are signs
There are two main criteria that report the likelihood of a fracture - relative and absolute.
Relative signs of a fracture:
Pain that gradually increases significantly at the site of the injury.
After some time, a hematoma appears in the area of the fracture. If it also pulsates, this may indicate that intense bleeding continues inside the damaged area.
The shape of the limb changes.
The damaged limb loses its inherent functions, for example, its mobility or ability to withstand previously permissible loads is limited.
Swelling occurs in the area of damage.
Absolute signs of a fracture:
Bone fragments can be seen in the wound.
The presence of a peculiar crunching sound called crepitus. This crunch can be heard by placing your ear to the damaged area, and sometimes it can be felt just at your fingertips.
The position of the limb is unnatural.
Abnormal mobility, i.e. the limb becomes mobile in the place where there is no joint.
Clinically, symptoms of a fracture can be divided into reliable and probable. The first include: a feeling of crunching of bone fragments at the fracture site and the occurrence of pathological mobility. The second includes pain, hematoma, deformation, bruising, dysfunction and swelling.
You should always pay close attention to the color of the skin directly around the injured area, as well as in the area of the hand and foot. If you notice severe paleness of the skin, a bluish tint without any movement, this may indicate damage to large vessels. Serious damage may also be indicated by loss of skin sensitivity, unpleasant burning sensation, lack of pulse in the damaged area, “pins and needles” sensation, tingling.
In all of the above cases, you should immediately seek help from a doctor.
Fractures are a pathological condition in which bone deformation occurs under the influence of a damaging factor that exceeds the strength of bone tissue. Injuries are more common in childhood and old age, which is associated with the anatomical and physiological characteristics of the body.
A child's bones are more elastic and less durable than those of adults. This causes the skeleton to be vulnerable to traumatic factors. The high risk of fractures in children is associated with the child’s mobility and poor development of self-preservation skills. In older people, due to age-related changes, calcium salts are washed out of the bones, which leads to osteoporosis and a decrease in skeletal strength. Violation cerebral circulation, leading to poor balance and dizziness, causing unsteady gait and frequent falls.
In young people, the risk of bone deformation is associated with seasonality (ice), professional activity (intense physical exercise), sports (professional athletes). In modern international classification diseases (abbreviated as ICD 10), fractures are assigned class 19 - injuries, poisoning and other consequences when exposed to external factors.
Classification
The classification of fractures was created to simplify diagnosis, determine treatment tactics and prognosis of the disease. Injuries are distinguished by etiology (reason of origin), form of bone defect, displacement of bone fragments, formation of bone fragments and other factors. We will look at what types of fractures there are below and present different classifications of skeletal injuries.

From left to right there is a fracture inside the joint, open and closed injury
Fractures are classified based on the reason they occur:
- traumatic – occur when healthy bones with a sufficient degree of strength are exposed to an intense traumatic factor;
- pathological - occur when a traumatic factor of insignificant damaging force is exposed to pathologically altered bones with low strength potential.
Traumatic bone defects appear due to a direct blow, a fall from a height, violent actions, awkward movements, or gunshot wounds. Such fractures are called straight. Sometimes the place where the force is applied and the area where the injury occurs may be located at some distance. These are indirect fractures. Pathological bone defects occur against the background of diseases that lead to weakening of bone tissue and reduce its strength. A high risk of skeletal injuries is caused by bone cysts, tumors or metastases, osteomyelitis, osteoporosis, impaired osteogenesis during embryonic development, and chronic wasting diseases.
Based on the communication between bone fragments and the environment, fractures are distinguished:
- open – accompanied by damage to the external integument;
- closed - occur without the formation of a wound.
Open bone defects can be primary or secondary. Primary ones are characterized by the formation of a wound when exposed to a traumatic factor. Secondary ones appear after the moment of injury as a result of the cutting of the skin by the sharp edges of the bones due to improper transportation of the patient to the emergency room or unsuccessful repositioning of the bone during treatment.

Bone fractures differ in the direction of the bone defect line
Closed fractures are:
- incomplete – formed like a crack without displacement of bone fragments;
- complete - characterized by complete separation of the ends of the bone and displacement in different sides;
- single – injury to one bone;
- multiple – injury to several bones;
- combined – the occurrence of a bone defect as a result of the influence of various negative factors (mechanical, radiation, chemical);
- combined – skeletal injuries are combined with damage to visceral organs.
Incomplete fractures occur due to exposure to minor traumatic forces. More often, such defects occur in children whose bones are covered with a thick and elastic periosteum. The child is characterized by injuries of the “green stick” type – bone cracks without displacement of fragments. Incomplete defects include marginal and perforated fractures, fractures and cracks. Complete separation of bone fragments develops when a significant impact force is applied or a defect is formed in areas of bones with well-developed muscles. Muscle contraction leads to displacement of bone fragments in different directions along the trajectory of muscle fiber traction.
A displaced fracture is considered a severe injury that requires long-term treatment and recovery period. Open injuries are also included in this group. In addition, they are accompanied by primary infection of the wound, which can lead to osteomyelitis and sepsis. Displacement of fragments of damaged bones causes the development of complications associated with damage muscle tissue, nerves and blood vessels.

Fracture inside a joint
As a result, open and closed bleeding, impaired innervation of the limbs, paralysis and decreased sensitivity occur. Damage to soft tissues and large blood vessels leads to pain and hemorrhagic shock, which complicates the treatment of injury and can cause fatal outcome. A fracture without displacement usually does not lead to undesirable consequences and in most cases has a favorable outcome.
Based on the location of the bone defect, the following types of fractures are distinguished:
- formation in the lower, middle or upper third of the bone (in case of injuries to tubular bones);
- impacted or impression (in case of injuries to spongy bones, for example, vertebrae);
- diaphyseal (located between the ends of the tubular bones);
- metaphyseal (located near the joints);
- epiphyseal (located in the joint cavity);
- epiphysiolysis (in the bone growth zone in childhood).
Epipharic injuries can occur as fracture-dislocations, which complicates the treatment of the disease and lengthens the rehabilitation period. Epiphysiolysis with inadequate therapy contributes to the premature closure of skeletal growth zones and causes shortening of the damaged limb.
Depending on the shape of the bone defect line, the following types of fractures are distinguished:
- oblique,
- transverse,
- longitudinal,
- screw,
- splintered.
A comminuted fracture is accompanied by the formation of one or more bone fragments, which are completely separated from the bone and are located in the soft tissues. Such injuries require surgical treatment and a long period of rehabilitation. A comminuted fracture with the formation of multiple fragments is usually called comminuted. It causes a significant defect in the damaged bone. Comminuted fractures can be finely or coarsely comminuted.

Defects with a transverse fracture line are classified as stable injuries with rare displacement of bone fragments. Other types of fractures lead to displacement of fragments due to muscle traction after injury and are included in the group of unstable fractures. Proper transportation of the patient to the emergency room and adequate treatment methods prevent the development of complications due to displacement of bone fragments.
Classification of bone fractures helps to choose the right treatment tactics and prevent the development of undesirable consequences, predict the duration of therapy and rehabilitation period. Staging accurate diagnosis, according to modern classification, improves the prognosis of injury and reduces the risk of severe complications.
Consequences
After a fracture occurs, you must immediately seek medical help. In case of severe injuries, which are accompanied by the formation of a wound or displacement of damaged bones, bleeding, multiple lesions bones, deterioration of the general condition of the victim due to hemorrhagic and painful shock, an ambulance should be called. If it is impossible to call doctors, the patient is transported independently to the trauma department after treatment. first aid and application of transport tires.
With methods for using immobilization splints, rules for providing first aid and methods for treating fractures.

Internal blood loss leads to hematoma formation
Undesirable consequences of a fracture occur when the victim is transported incorrectly to the hospital, late seeking medical help, inadequate choice of therapy and violation of the treatment regimen. If you suspect an injury, you must consult a doctor, undergo X-ray diagnostics and promptly begin treatment if a bone defect is confirmed.
Outcomes of fracture healing:
- full recovery anatomical structure and functions of the injured leg or body part;
- complete restoration of the anatomical structure with limited functionality;
- improper fusion of bones with dysfunction of a limb or part of the body (deformation, shortening of the limb);
- Non-union of bone fragments with formation.
Complications that arise after healing of the injury depend on the correct reposition (comparison) of fragments and sufficient fixation of the bone, concomitant soft tissue damage, rehabilitation measures and the duration of the period of limitation of motor activity. The types of bone fractures affect the healing time of the injury. Longer therapeutic immobilization is necessary for open injuries, closed injuries with bone displacement and the formation of bone fragments, as well as in the case of intra-articular disorders and the formation of fracture-dislocations.
Useful information on how to recognize fracture formation, clinical signs of injury and diagnosis of the disease.
Complications of fractures can be divided into 3 main groups:
- Static disorders of bone tissue (absence or improper healing, deformation or shortening of the leg, formation of a false joint).
- Soft tissue disorders (deterioration of blood flow and innervation, muscle atrophy, bleeding).
- Local infection at the site of injury (wound, bones) or spread of infection throughout the body (sepsis).

Limb deformity due to improper bone fusion
Unhealed bone fractures are formed when the fragments are incorrectly juxtaposed, as a result of which the formation of callus is disrupted. When soft tissue gets between the ends of a damaged bone, a false joint may occur, which leads to pathological mobility in the area of injury and impairment normal function limbs. Due to the pathology of bone consolidation, shortening or deformation of the limbs develops, which leads to disability.
Bleeding from large vessels when their integrity is violated by sharp edges of bones causes the development of bleeding. With a closed injury of the hip, the blood loss is 1-2 liters, the bones of the leg - 600-800 ml, the bones of the shoulder - 300-500 ml and the forearm - 100-250 ml. With open injuries in the area of large blood vessels (carotid, inguinal, femoral arteries and aorta), bleeding can cause significant blood loss (more than 2 liters) and lead to death.
Broken bones with damage nerve trunks causes disturbance motor function and sensitive areas. After the defect heals, a large callus, which compresses blood vessels and nerves. As a result, paralysis and paresis develop, congestion in tissues leading to disability.
Prolonged immobilization of the limb contributes to muscle atrophy and the formation of joint immobility (ankylosis). After removing the plaster, traction or external fixation device, a disturbance in the outflow of blood and lymph from the damaged area of the limb is observed, which causes swelling, bluishness of the skin and stiffness of the joints. To prevent the formation of undesirable consequences of limb fractures, adequate therapy is carried out and rehabilitation measures on different stages healing of injury.

Pseudarthrosis formation
Infectious complications are typical for open bone injuries. As a result of injury, pathogenic microorganisms enter the wound, which cause suppuration of soft tissues, bones (osteomyelitis) or generalization of infection (sepsis). Less commonly, ulcers form in the area of internal or external osteosynthesis (comparison of bones using knitting needles, plates, screws). To prevent infection, the wound is treated aseptically, the skin defect is sutured, and a course of antibiotics is prescribed.
Improper or prolonged healing of fractures causes scarring that puts pressure on blood vessels and nerves. This leads to chronic pain syndrome after consolidation of bone fragments and return to normal physical activity. Painful sensations worsen after long walks, heavy lifting, change weather conditions, can cause insomnia and mental exhaustion of the body. Significant decrease in working capacity due to constant pain leads to disability.
Bone fractures differ in various ways. To make an accurate diagnosis and select the correct treatment method, a classification was created that reflects specific features one or another injury. The consequences of fractures depend on the severity of the injury, timely provision of first aid, and correctly selected treatment and rehabilitation tactics. If you follow your doctor's recommendations, in most cases clinical cases it is possible to completely restore the anatomical integrity of the damaged bone and the functional activity of a limb or part of the body.
Types and signs of fractures. Signs of dislocations in the joints. Rules and methods of providing first aid for bone fractures and dislocations. Rules for applying splints. Application of splints and immobilization of joints for certain types of fractures and dislocations using standard and improvised means
Types and signs of fractures
1. Types of fractures. Fractures can be closed, in which the integrity of the skin is not broken, there is no wound, and open, when the fracture is accompanied by injury to soft tissue.
Depending on the degree of damage, a fracture can be complete, in which the bone is completely broken, and incomplete, when there is only a fracture or crack in the bone. Complete fractures are divided into fractures with displacement and without displacement of bone fragments.
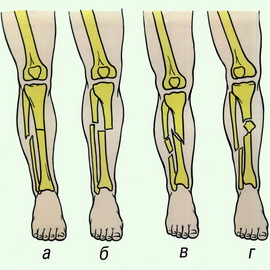
Based on the direction of the fracture line relative to the long axis of the bone, transverse (a), oblique (b) and helical (c) fractures are distinguished. If the force that caused the fracture was directed along the bone, then its fragments can be pressed into one another. Such fractures are called impacted.
When damaged by bullets and fragments flying at high speed and possessing great energy, many bone fragments are formed at the fracture site - a comminuted fracture is obtained (e).
Fractures: a - transverse; b - oblique: c - helical; g - driven in; d - splintered
Signs of bone fractures. With the most common fractures of the bones of the limb, severe swelling, bruising, and sometimes bending of the limb outside the joint and shortening appear in the area of injury. In the case of an open fracture, the ends of the bone may protrude from the wound. The site of injury is sharply painful. In this case, it is possible to determine abnormal mobility of the limb outside the joint, which is sometimes accompanied by a crunching sound from the friction of bone fragments. It is unacceptable to specifically bend a limb to make sure there is a fracture - this can lead to dangerous complications. In some cases, with bone fractures, not all of the indicated signs are revealed, but the most characteristic are severe pain and severe difficulty in moving.
A rib fracture can be assumed when, due to a bruise or compression of the chest, the victim notices severe pain when deep breathing, as well as when feeling the site of a possible fracture. If the pleura or lung is damaged, bleeding occurs or air enters the chest cavity. This is accompanied by respiratory and circulatory disorders.
In case of a spinal fracture, severe back pain, paresis and paralysis of the muscles below the fracture site appear. Involuntary loss of urine and feces may occur due to dysfunction of the spinal cord.
When the pelvic bones are fractured, the victim cannot stand up, raise his legs, or turn around. These fractures are often combined with damage to the intestines and bladder.
Bone fractures are dangerous due to damage to the blood vessels and nerves located near them, which is accompanied by bleeding, loss of sensitivity and movement in the damaged area.
Severe pain and bleeding can cause the development of shock, especially if the fracture is not immobilized in a timely manner. Bone fragments can also damage the skin, as a result of which a closed fracture turns into an open one, which is dangerous due to microbial contamination. Movement at the fracture site can lead to serious complications, so it is necessary to immobilize the damaged area as quickly as possible.
2. Signs of joint dislocations
A dislocation is a displacement of the articular ends of bones. This is often accompanied by rupture of the joint capsule. Dislocations are often observed in the shoulder joint, in the joints of the lower jaw, and fingers. With a dislocation, three main signs are observed: complete impossibility of movement in the damaged joint, severe pain; forced situation limbs, caused by muscle contraction (for example, when a shoulder is dislocated, the victim keeps his arm bent at the elbow joint and abducted to the side); change in the configuration of the joint compared to the joint on the healthy side.
There is often swelling in the joint area due to hemorrhage. Articular head It is not possible to palpate in the usual place; in its place the glenoid cavity is determined.
3. Rules and methods of providing first aid for bone fractures and dislocations
General rules for providing first aid for bone fractures.
To examine the fracture site and apply a bandage to the wound (in the case of an open fracture), clothing and shoes are not removed, but cut. First of all, stop the bleeding and apply an aseptic bandage. Then the affected area is given comfortable position and apply an immobilizing bandage.
An anesthetic is injected under the skin or intramuscularly from a syringe tube.
To immobilize fractures, standard splints contained in the B-2 kit or improvised means are used.
First aid for dislocations consists of fixing the limb in a position that is most comfortable for the victim, using a splint or bandage. A doctor must correct the dislocation. A dislocation in a particular joint may recur periodically (habitual dislocation).
4. Rules for applying splints. Application of splints and immobilization of joints for certain types of fractures and dislocations using standard and improvised means
General rules for applying splints for fractures of extremity bones.
- the splints must be securely fastened, well fixing the fracture area;
- the splint cannot be applied directly to a naked limb; the latter must first be covered with cotton wool or some kind of cloth;
- creating immobility in the fracture zone, it is necessary to fix two joints above and below the fracture site (for example, in case of a tibia fracture, the ankle and knee joints are fixed) in a position convenient for the patient and for transportation;
In case of hip fractures, all joints of the lower limb (knee, ankle, hip) should be fixed.
First aid for hip fractures. General rules for applying splints
Hip injuries are usually accompanied by significant blood loss. Even with a closed fracture of the femur, blood loss into the surrounding soft tissue is up to 1.5 liters. Significant blood loss contributes to frequent development shock.
Main signs of hip injuries:
- pain in the hip or joints, which sharply increases with movement;
- movements in the joints are impossible or significantly limited;
- with hip fractures, its shape is changed and abnormal mobility at the fracture site is determined, the femur is shortened;
- movements in the joints are impossible;
- lack of sensitivity in the peripheral parts of the leg.
The best standard splint for hip injuries is the Dieterichs splint.
Immobilization will be more reliable if the Dieterichs splint is reinforced with plaster rings in the area of the torso, thigh and lower leg in addition to the usual fixation. Each ring is formed by applying 7-8 circular rounds of plaster bandage. There are 5 rings in total: 2 on the torso, 3 on the lower limb.
In the absence of a Dieterichs splint, immobilization is performed using ladder splints.
![]()
Immobilization with ladder splints. To immobilize the entire lower limb, four ladder splints, each 120 cm long, are required; if the splints are not sufficient, it is possible to immobilize with three splints.
The tires must be carefully wrapped with a layer of gray wool of the required thickness and bandages. One splint is curved along the contour of the back of the thigh, lower leg and foot to form a recess for the heel and calf muscles.
In an area intended for popliteal region, arching is performed in such a way that the leg is slightly bent at the knee joint. The lower end is bent in the shape of the letter “G” to fix the foot in a position of flexion at the ankle joint at a right angle, while the lower end of the splint should grip the entire foot and protrude 1-2 cm beyond the fingertips.
The other two tires are tied together along the length, the lower end is bent in an L-shape at a distance of 15-20 cm from the lower edge. An elongated splint is placed along the outer surface of the torso and limbs from the axillary region to the foot. The lower curved end wraps the foot over the rear tire to prevent foot drop.
The fourth splint is placed along the inner lateral surface of the thigh from the perineum to the foot. Its lower end is also bent in the shape of the letter “L” and placed behind the foot over the curved lower end of the elongated outer side splint. The splints are reinforced with gauze bandages.
Likewise, in the absence of other standard splints, as a necessary measure, the lower limb can be immobilized with plywood splints.
At the first opportunity, ladder and plywood tires should be replaced with a Dieterichs tire.
Mistakes when immobilizing the entire lower limb with ladder splints:
1. Insufficient fixation of the external extended splint to the body, which does not allow reliable immobilization hip joint. In this case, immobilization will be ineffective.
2. Poor modeling of the rear ladder tire. There is no recess for calf muscle and heels. There is no bending of the splint in the popliteal region, as a result of which the lower limb is immobilized completely straightened in the knee joint, which in case of hip fractures can lead to compression of large vessels by bone fragments.
3. Plantar drop of the foot as a result of insufficiently strong fixation (there is no modeling of the lower end of the side splints in the form of the letter “L”).
4. Not enough thick layer cotton wool on the splint, especially in the area of bony protrusions, which can lead to the formation of bedsores.
5. Compression of the lower limb due to tight bandaging.
Transport immobilization using improvised means for hip injuries: a - from narrow boards; b - using skis and ski poles.
Immobilization using improvised means. Performed in the absence of standard tires. For immobilization, wooden slats, skis, branches and other objects of sufficient length are used to ensure immobilization in three joints of the injured lower limb (hip, knee and ankle). The foot must be placed at a right angle at the ankle joint and pads made of soft material must be used, especially in the area of the bony protrusions.
In cases where there are no means for transport immobilization, the “leg to leg” fixation method should be used. The damaged limb is tied in two or three places to the healthy leg, or the damaged limb is placed on the healthy one and also tied in several places.
Transport immobilization for injuries of the lower extremities using the “foot to foot” method: a - simple immobilization; b - immobilization with light traction
Immobilization of the injured limb using the “foot-to-foot” method should be replaced by immobilization with standard splints as soon as possible.
Evacuation of victims with hip injuries is carried out on a stretcher in a lying position. To prevent and timely identify complications of transport immobilization, it is necessary to monitor the state of blood circulation in the peripheral parts of the limb. If the limb is bare, then monitor the color of the skin. If clothes and shoes are not removed, it is necessary to pay attention to the victim’s complaints. Numbness, coldness, tingling, increased pain, the appearance of throbbing pain, cramps in the calf muscles are signs of poor circulation in the limb. It is necessary to immediately loosen or cut the bandage at the point of compression.
First aid for shin fractures. General rules for applying splints
Main signs of shin injuries:
- pain at the site of injury, which intensifies with movement of the injured leg;
- deformation at the site of injury to the lower leg;
- movements in the ankle joint are impossible or significantly limited;
- extensive bruising in the area of injury.
Immobilization is best achieved by an L-shaped curved modeled posterior ladder tire 120 cm long and two side ladder or plywood tires 80 cm long. The upper end of the tires should reach the middle of the thigh. The lower end of the side stair rails is bent L-shaped. The leg is slightly bent at the knee joint. The foot is positioned at a right angle to the shin. The splints are reinforced with gauze bandages.
Immobilization can be performed with two 120 cm long stair splints.
Errors in transport immobilization of lower leg injuries using ladder splints:
1. Insufficient modeling of the scalene splint (there is no recess for the heel and calf muscles, there is no arching of the splint in the popliteal region).
2. Immobilization is performed only with the rear ladder splint without additional lateral splints.
3. Insufficient fixation of the foot (the lower end of the side splints is not bent L-shaped), which leads to plantar sagging.
4. Insufficient immobilization of the knee and ankle joints.
5. Compressing the leg with a tight bandage while strengthening the splint.
6. Fixation of the limb in a position where the tension of the skin over the bone fragments remains (the front surface of the leg, ankle), which leads to damage to the skin over the bone fragments or the formation of bedsores. Skin tension caused by displaced bone fragments in the upper half of the leg is eliminated by immobilizing the knee joint in a position of full extension.
Immobilization of lower leg injuries with three ladder splints: a - preparation of ladder splints; b - application and fixation of splints
![]()
![]()
Immobilization of lower leg injuries in the absence of standard splints can be performed using improvised means.
First aid for shoulder fractures. General rules for applying splints
Signs of shoulder fractures and damage to adjacent joints:
- severe pain and swelling in the area of injury;
- pain increases sharply with movement;
- change in the shape of the shoulder and joints;
- movements in the joints are significantly limited or impossible;
- abnormal mobility in the area of the shoulder fracture.
Immobilization with a ladder splint is the most effective and reliable way transport immobilization for shoulder injuries.
The splint should cover the entire injured limb - from the shoulder blade of the healthy side to the hand on the injured arm and at the same time protrude 2-3 cm beyond the fingertips. Immobilization is performed using a ladder splint 120 cm long.
The upper limb is immobilized in the position of slight anterior and lateral abduction of the shoulder. To do this in axillary area a ball of cotton is placed on the injured side, the elbow joint is bent at a right angle, the forearm is positioned so that the palm of the hand is facing the stomach. A cotton roller is placed into the brush.
Preparing the tire
Measure the length from the outer edge of the victim’s shoulder blade to the shoulder joint and bend the splint at an obtuse angle at this distance;
Measure the distance from the upper edge of the shoulder joint to the elbow joint along the back surface of the victim’s shoulder and bend the splint at this distance at a right angle;
The person providing assistance additionally bends the splint along the contours of the back, back of the shoulder and forearm.
It is recommended to bend the part of the splint intended for the forearm into the shape of a groove.
Having tried the curved splint on the victim’s healthy arm, the necessary corrections are made.
If the tire is not long enough and the brush hangs down, its lower end must be extended with a piece of plywood tire or a piece of thick cardboard. If the length of the tire is excessive, its lower end is bent.
Two gauze ribbons 75 cm long are tied to the upper end of the splint wrapped in gray cotton wool and bandages.
The splint prepared for use is applied to the injured arm, the upper and lower ends of the splint are tied with braids and the splint is strengthened with bandages. The arm along with the splint is suspended on a scarf or sling.
To improve fixation of the upper end of the splint, attach two additional pieces of bandage 1.5 m long to it, then pass the bandage around the shoulder joint of the healthy limb, make a cross, circle it around the chest and tie it.
![]()
Transport immobilization of the entire upper limb with a ladder splint:
a - applying a splint to the upper limb and tying its ends;
b - strengthening the splint with bandaging; c - hanging a hand on a scarf
When immobilizing the shoulder with a ladder splint, the following errors are possible:
1. The upper end of the splint reaches only the shoulder blade of the affected side; very soon the splint moves away from the back and rests on the neck or head. With this position of the splint, immobilization of injuries to the shoulder and shoulder joint will be insufficient.
2. The absence of ribbons at the upper end of the tire, which does not allow it to be securely fixed.
3. Poor tire modeling.
4. The immobilized limb is not suspended from a scarf or sling.
In the absence of standard splints, immobilization is carried out using a medical scarf, improvised means or soft bandages.
Immobilization with a medical scarf. Immobilization with a scarf is carried out in the position of slight anterior abduction of the shoulder with the elbow joint bent at a right angle. The base of the scarf is wrapped around the body approximately 5 cm above the elbow and its ends are tied on the back closer to the healthy side. The top of the scarf is placed upward on the shoulder girdle of the injured side. The resulting pocket holds the elbow joint, forearm and hand.
The top of the scarf on the back is tied to the longer end of the base. The damaged limb is completely covered by a scarf and fixed to the body.
Immobilization using improvised means. Several planks and a piece of thick cardboard in the form of a trench can be laid on the inner and outer surfaces of the shoulder, which creates some immobility during a fracture. The hand is then placed on a scarf or supported by a sling.
Immobilization with Deso bandage. In extreme cases, immobilization for shoulder fractures and damage to adjacent joints is carried out by bandaging the limb to the body with a Deso bandage.
Properly performed immobilization of the upper limb significantly alleviates the condition of the victim and special care during evacuation, as a rule, is not required. However, the limb should be periodically examined so that if swelling in the area of injury increases, compression does not occur. To monitor the state of blood circulation in the peripheral parts of the limb, it is recommended to leave the terminal phalanges of the fingers unbandaged. If signs of compression appear, the bandage should be loosened or cut and bandaged.
Transportation is carried out in a sitting position, if the condition of the victim allows.
First aid for forearm fractures. General rules for applying splints
Signs of forearm bone fractures:
- pain and swelling in the area of injury;
- pain increases significantly with movement;
- movements of the injured arm are limited or impossible;
- change in the normal shape and volume of the forearm joints;
- abnormal mobility in the area of injury.
Immobilization with a ladder splint is the most reliable and effective type of transport immobilization for injuries of the forearm.
The ladder splint is applied from the upper third of the shoulder to the fingertips, the lower end of the splint stands at 2-3 cm. The arm should be bent at the elbow joint at a right angle, and the hand should be facing the stomach and slightly retracted to the back; cotton wool should be placed in the hand. a gauze roller to hold the fingers in a semi-flexed position.
A ladder splint 80 cm long, wrapped in gray cotton wool and bandages, is bent at a right angle at the level of the elbow joint so that the upper end of the splint is at the level of the upper third of the shoulder; the section of the splint for the forearm is bent in the form of a groove. Then they apply it to the healthy hand and correct the defects of the modeling. The prepared splint is applied to the sore arm, bandaged along its entire length and hung on a scarf.
The upper part of the splint intended for the shoulder must be of sufficient length to reliably immobilize the elbow joint. Insufficient fixation of the elbow joint makes immobilization of the forearm ineffective.
In the absence of a ladder splint, immobilization is carried out using a plywood splint, a plank, a scarf, a bundle of brushwood, or the hem of a shirt.
Transport immobilization of the forearm:
a - ladder tire; b - using improvised means (using planks)
First aid for sprained limbs
The most common traumatic dislocations are caused by excessive movement in the joint. This happens, for example, when strong impact in the joint area, fall. As a rule, dislocations are accompanied by rupture of the joint capsule and separation of the articular surfaces. An attempt to compare them does not bring success and is accompanied by severe pain and springy resistance. Sometimes dislocations are complicated by fractures - fracture-dislocations. Reduction of a traumatic dislocation should be as early as possible.
Help with sprains.
Since any, even minor, movement of a limb brings unbearable pain, first of all, it is necessary to fix the limb in the position in which it finds itself, ensuring its rest during the hospitalization stage. For this purpose, transport tires, special bandages or any available means are used. To immobilize the upper limb, you can use a scarf, the narrow ends of which are tied across the neck.
If the lower limb is dislocated, splints or boards are placed under it and on the sides and the limb is bandaged to them.
If the fingers of the hand are dislocated, the entire hand is immobilized to any flat, hard surface. In the area of the joints, a layer of cotton wool is laid between the splint and the limb.
When the lower jaw is dislocated, a sling-shaped bandage is placed under it (reminiscent of a bandage put on the hand of an attendant), the ends of which are tied crosswise at the back of the head.
After applying a splint or fixing bandage, the victim must be hospitalized to reduce the dislocation.




