Time frame for the formation of roots of permanent teeth in children. General assessment of radiographs. Dental pulp development
Phylogenetically, the root arose later than the stem and leaf - in connection with the transition of plants to life on land and probably originated from root-like underground branches. The root has neither leaves nor buds arranged in a certain order. It is characterized by apical growth in length, its lateral branches arise from internal tissues, the growth point is covered with a root cap. The root system is formed throughout life plant organism. Sometimes the root can serve as a storage site for nutrients. In this case, it changes.
Types of roots
The main root is formed from the embryonic root during seed germination. Lateral roots extend from it.
Adventitious roots develop on stems and leaves.
Lateral roots are branches of any roots.
Each root (main, lateral, adventitious) has the ability to branch, which significantly increases the surface of the root system, and this contributes to better strengthening plants in the soil and improving its nutrition.
Types of root systems
There are two main types of root systems: taproot, which has a well-developed main root, and fibrous. The fibrous root system consists of large number adventitious roots of equal size. The entire mass of roots consists of lateral or adventitious roots and has the appearance of a lobe.
The highly branched root system forms a huge absorbent surface. For example,
- the total length of winter rye roots reaches 600 km;
- length of root hairs - 10,000 km;
- the total root surface is 200 m2.
This is many times the area of the aboveground mass.

If the plant has a well-defined main root and adventitious roots develop, then a mixed type root system (cabbage, tomato) is formed.
External structure of the root. Internal structure of the root
Root zones

Root cap
The root grows in length from its apex, where the young cells of the educational tissue are located. The growing part is covered with a root cap, which protects the root tip from damage and facilitates the movement of the root in the soil during growth. The latter function is carried out due to the property of the outer walls of the root cap being covered with mucus, which reduces friction between the root and soil particles. They can even push soil particles apart. The cells of the root cap are living and often contain starch grains. The cells of the cap are constantly renewed due to division. Participates in positive geotropic reactions (direction of root growth towards the center of the Earth).

The cells of the division zone are actively dividing; the extent of this zone varies in different species and in different roots of the same plant.
Behind the division zone is an extension zone (growth zone). The length of this zone does not exceed a few millimeters.
As linear growth completes, the third stage of root formation begins—its differentiation; a zone of cell differentiation and specialization (or a zone of root hairs and absorption) is formed. In this zone, the outer layer of the epiblema (rhizoderm) with root hairs, the layer of the primary cortex and the central cylinder are already distinguished.
Root hair structure
Root hairs are highly elongated outgrowths of the outer cells covering the root. The number of root hairs is very large (per 1 mm2 from 200 to 300 hairs). Their length reaches 10 mm. Hairs form very quickly (in young apple tree seedlings in 30-40 hours). Root hairs are short-lived. They die off after 10-20 days, and new ones grow on the young part of the root. This ensures the development of new soil horizons by the roots. The root continuously grows, forming more and more new areas of root hairs. Hairs can not only absorb ready-made solutions of substances, but also contribute to the dissolution of certain soil substances and then absorb them. The area of the root where the root hairs have died is able to absorb water for a while, but then becomes covered with a plug and loses this ability.
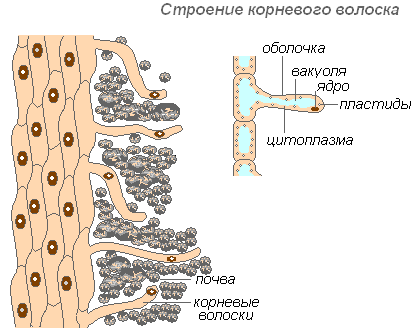
The hair shell is very thin, which facilitates the absorption of nutrients. Almost the entire hair cell is occupied by a vacuole, surrounded by a thin layer of cytoplasm. The nucleus is at the top of the cell. A mucous sheath is formed around the cell, which promotes the gluing of root hairs to soil particles, which improves their contact and increases the hydrophilicity of the system. Absorption is facilitated by the secretion of acids (carbonic, malic, citric) by root hairs, which dissolve mineral salts.
Root hairs also play a mechanical role - they serve as support for the root tip, which passes between the soil particles.
Under a microscope, a cross section of the root in the absorption zone shows its structure at the cellular and tissue levels. On the surface of the root there is rhizoderm, under it there is bark. The outer layer of the cortex is the exodermis, inward from it is the main parenchyma. Its thin-walled living cells perform a storage function, conducting nutrient solutions in a radial direction - from the suction tissue to the vessels of the wood. They also contain the synthesis of a number of organic substances vital for the plant. The inner layer of the cortex is the endoderm. Nutrient solutions entering the central cylinder from the cortex through endodermal cells pass only through the protoplast of cells.
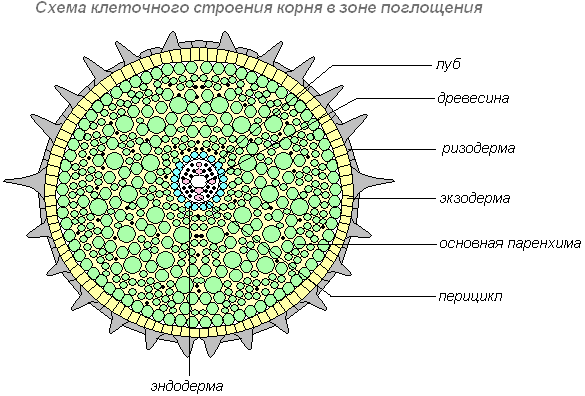
The bark surrounds the central cylinder of the root. It borders on a layer of cells that retain the ability to divide for a long time. This is a pericycle. Pericycle cells give rise to lateral roots, adventitious buds and secondary educational tissues. Inward from the pericycle, in the center of the root, there are conductive tissues: bast and wood. Together they form a radial conductive bundle.
The root vascular system conducts water and minerals from the root to the stem (upward current) and organic matter from the stem to the root (downward current). It consists of vascular-fibrous bundles. The main components of the bundle are sections of the phloem (through which substances move to the root) and xylem (through which substances move from the root). The main conducting elements of phloem are sieve tubes, xylem is trachea (vessels) and tracheids.
Root life processes
Transport of water in the root
Absorption of water by root hairs from the soil nutrient solution and conduction of it in a radial direction along the cells of the primary cortex through passage cells in the endoderm to the xylem of the radial vascular bundle. The intensity of water absorption by root hairs is called suction force (S), it is equal to the difference between osmotic (P) and turgor (T) pressure: S=P-T.
When the osmotic pressure is equal to the turgor pressure (P=T), then S=0, water stops flowing into the root hair cell. If the concentration of substances in the soil nutrient solution is higher than inside the cell, then water will leave the cells and plasmolysis will occur - the plants will wither. This phenomenon is observed in dry soil conditions, as well as with excessive application. mineral fertilizers. Inside the root cells, the suction force of the root increases from the rhizoderm towards the central cylinder, so water moves along a concentration gradient (i.e. from a place with a higher concentration to a place with a lower concentration) and creates root pressure, which raises the column of water through the xylem vessels , forming an ascending current. This can be found on leafless trunks in the spring when the “sap” is collected, or on cut stumps. The flow of water from wood, fresh stumps, and leaves is called “crying” of plants. When the leaves bloom, they also create a suction force and attract water to themselves - a continuous column of water is formed in each vessel - capillary tension. Root pressure is the lower driver of water flow, and the suction force of the leaves is the upper one. This can be confirmed using simple experiments.
Absorption of water by roots
Target: find out the basic function of the root.
What we do: plant grown on wet sawdust, shake off its root system and lower its roots into a glass of water. To protect it from evaporation, pour a thin layer of vegetable oil on top of the water and mark the level.

What we see: After a day or two, the water in the container dropped below the mark.

Result: consequently, the roots sucked up the water and brought it up to the leaves.
You can also do one more experiment to prove the absorption of nutrients by the root.
What we do: cut off the stem of the plant, leaving a stump 2-3 cm high. We put a rubber tube 3 cm long on the stump, and top end put on a curved glass tube 20-25 cm high.
What we see: The water in the glass tube rises and flows out.
Result: this proves that the root absorbs water from the soil into the stem.

Does water temperature affect the intensity of water absorption by roots?
Target: find out how temperature affects root function.
What we do: one glass should be with warm water(+17-18ºС), and the other with cold (+1-2ºС).
What we see: in the first case, water is released abundantly, in the second - little, or stops altogether.
Result: this is proof that temperature greatly influences root function.

Warm water is actively absorbed by the roots. Root pressure increases.

Cold water is poorly absorbed by the roots. In this case, root pressure drops.
Mineral nutrition
The physiological role of minerals is very great. They are the basis for the synthesis of organic compounds, as well as factors that change physical state colloids, i.e. directly affect the metabolism and structure of the protoplast; act as catalysts for biochemical reactions; affect cell turgor and protoplasm permeability; are centers of electrical and radioactive phenomena in plant organisms.
It has been established that normal plant development is possible only if there are three non-metals in the nutrient solution - nitrogen, phosphorus and sulfur and four metals - potassium, magnesium, calcium and iron. Each of these elements has an individual meaning and cannot be replaced by another. These are macroelements, their concentration in the plant is 10 -2 -10%. For normal plant development, microelements are needed, the concentration of which in the cell is 10 -5 -10 -3%. These are boron, cobalt, copper, zinc, manganese, molybdenum, etc. All these elements are present in the soil, but sometimes in insufficient quantities. Therefore, mineral and organic fertilizers are added to the soil.
The plant grows and develops normally if the environment surrounding the roots contains all the necessary nutrients. This environment for most plants is soil.
Breathing of roots
For normal height and the development of the plant, it is necessary for the root to receive Fresh air. Let's check if this is true?
Target: Does the root need air?
What we do: Let's take two identical vessels with water. Place developing seedlings in each vessel. Every day we saturate the water in one of the vessels with air using a spray bottle. Pour a thin layer of vegetable oil onto the surface of the water in the second vessel, as it delays the flow of air into the water.

What we see: After some time, the plant in the second vessel will stop growing, wither, and eventually die.

Result: The death of the plant occurs due to a lack of air necessary for the root to breathe.
Root modifications
Some plants store reserve nutrients in their roots. They accumulate carbohydrates, mineral salts, vitamins and other substances. Such roots grow greatly in thickness and acquire an unusual appearance. Both the root and the stem are involved in the formation of root crops.
Roots
If reserve substances accumulate in the main root and at the base of the stem of the main shoot, root vegetables (carrots) are formed. Plants that form root crops are mostly biennials. In the first year of life, they do not bloom and accumulate a lot of nutrients in the roots. On the second, they quickly bloom, using the accumulated nutrients and forming fruits and seeds.
Root tubers

In dahlia, reserve substances accumulate in adventitious roots, forming root tubers.
Bacterial nodules
The lateral roots of clover, lupine, and alfalfa are peculiarly changed. Bacteria settle in young lateral roots, which promotes the absorption of gaseous nitrogen from the soil air. Such roots take on the appearance of nodules. Thanks to these bacteria, these plants are able to live in nitrogen-poor soils and make them more fertile.
Stilates

Ramp, which grows in the intertidal zone, develops stilted roots. They hold large leafy shoots on unstable muddy soil high above the water.
Air
Tropical plants living on tree branches develop aerial roots. They are often found in orchids, bromeliads, and some ferns. Aerial roots hang freely in the air without reaching the ground and absorb moisture from rain or dew that falls on them.
Retractors
In bulbous and corm plants, such as crocuses, among the numerous thread-like roots there are several thicker, so-called retractor roots. By contracting, such roots pull the corm deeper into the soil.
Columnar

Ficus plants develop columnar above-ground roots, or support roots.
Soil as a habitat for roots
Soil for plants is the medium from which it receives water and nutrients. The amount of minerals in the soil depends on the specific characteristics of the parent rock, the activity of organisms, the life activity of the plants themselves, and the type of soil.
Soil particles compete with roots for moisture, retaining it on their surface. This is the so-called bound water, which is divided into hygroscopic and film water. It is held in place by the forces of molecular attraction. The moisture available to the plant is represented by capillary water, which is concentrated in the small pores of the soil.
An antagonistic relationship develops between moisture and the air phase of the soil. The more large pores there are in the soil, the better the gas regime of these soils, the less moisture the soil retains. The most favorable water-air regime is maintained in structural soils, where water and air exist simultaneously and do not interfere with each other - water fills the capillaries inside the structural units, and air fills the large pores between them.
The nature of the interaction between plant and soil is largely related to the absorption capacity of the soil - the ability to hold or bind chemical compounds.
Soil microflora decomposes organic matter into simpler compounds and participates in the formation of soil structure. The nature of these processes depends on the type of soil, chemical composition plant residues, physiological properties microorganisms and other factors. Soil animals take part in the formation of soil structure: annelids, insect larvae, etc.
As a result of a combination of biological and chemical processes in the soil, a complex complex of organic substances is formed, which is combined with the term “humus”.
Water culture method
What salts the plant needs, and what effect they have on its growth and development, was established through experience with aquatic crops. The water culture method is the cultivation of plants not in soil, but in aqueous solution mineral salts. Depending on the goal of the experiment, you can exclude a particular salt from the solution, reduce or increase its content. It was found that fertilizers containing nitrogen promote plant growth, those containing phosphorus promote the rapid ripening of fruits, and those containing potassium promote the rapid outflow of organic matter from leaves to roots. In this regard, it is recommended to apply fertilizers containing nitrogen before sowing or in the first half of summer; those containing phosphorus and potassium - in the second half of summer.
Using the water culture method, it was possible to establish not only the plant’s need for macroelements, but also to clarify the role of various microelements.
Currently, there are cases where plants are grown using hydroponics and aeroponics methods.
Hydroponics is the growing of plants in containers filled with gravel. Nutrient solution containing necessary elements, is fed into the vessels from below.
Aeroponics is the air culture of plants. With this method, the root system is in the air and is automatically (several times within an hour) sprayed weak solution nutrient salts.
Laying of the rudiments of milk and permanent teeth, mineralization, eruption of milk teeth and resorption of their roots, eruption of permanent teeth and the formation of their roots proceeds in a certain sequence and at certain times. The formation, development and eruption of teeth is directly dependent on the general condition of the child’s body and the nature of nutrition.
Full development of the roots of permanent teeth, according to the literature, ends in the following periods: central and lateral incisors - at the 10th year of life, canines and small molars - at 12-14 years, first molars - at 10 years, second molars - at 14 -16 years.
To determine the degree of development of the roots of permanent teeth at different ages and clarify the timing of the end of the formation of the root apex, we studied 2087 radiographs of the lower jaw in children and adolescents aged 4 to 18 years (there were 600 children aged 3 to 7 years, from 8 to 18 years - 1287 children). The clarification of these terms is dictated by the fact that the treatment method for pulp diseases depends primarily on whether the growth of the tooth root has finished and whether its apex has finally formed.
We consider the end of growth and formation of tooth roots to be the period when the apical foramen narrows to a minimum limit and the surrounding periapical zone consists of periodontal tissue approximately 0.25 mm thick, followed by alveolar bone. On the radiograph, in the presence of a fully formed root, we no longer mark the openings of the apex, and in its circumference we clearly distinguish only the periodontium and the bone tissue of the alveoli.
The timing of the completion of the formation of permanent teeth is individual and subject to significant fluctuations. However, it should be noted that in a significant percentage of cases, complete root formation ends for the teeth we studied later than expected mentioned by various authors.
Complete formation of the root of the sixth tooth ends at the age of ten only in 67.8% of cases. In 4.4% of cases, the root is finally formed only at 12 years of age; the complete formation of the seventh tooth ends at 16 years of age, and in some cases at 17 years of age.
The formation of the roots of the third, fourth and fifth teeth does not end at 12 years of age, but much later.
In 36% of cases, we saw on the radiographs of 14-year-old children a still unformed root apex, and only on the radiographs of 15-year-olds and 16-year-olds could we see the fully formed apices of these teeth in all cases.
We pay special attention to the timing of the end of growth of the roots of the sixth and seventh teeth. In terms of the frequency of caries, the sixth teeth, as is known, occupy first place. Complicated caries in children school age mainly affects teeth. Therefore, in order to select the correct method of therapy, we consider it mandatory to have radiography in children in all cases of treatment of pulp disease. When the pulp and periodontium are diseased in teeth with incomplete root growth, further root formation slows down.
Taking into account the literature and our radiological data on the development of teeth, their growth and the timing of the end of root formation, we propose the following scheme for the development of permanent teeth.
Sixth tooth. The formation of the first permanent molar occurs in the 6th month of uterine life. IN last month In uterine life, the formation of dental shards begins, and mineralization centers appear. After 6 months of life, the individual centers stick together. The fusion of individual shards occurs along the edge of the crown, while its central part remains unmineralized. By 6 months of life, mineralization of approximately 1/4 of the crown is noted. By the 18th month, the crown of the sixth teeth reaches 2/3 of its length. By 3 years of age, signs of neck formation appear; by 4 years of age, the neck of the first molar is fully formed. By this time, the process of enamel formation reaches the enamel-cementum boundary. The enamel of the first permanent molar reaches its full development between the ages of 3 and 4 years. From this time, root formation begins; in the 6th year, the first permanent molar erupts. In early developing children, it erupts at 5 years of age, and sometimes, as we observed, at 4 years of age. By the age of 12, root growth ends; V exceptional cases this process drags on until 13-14 years.
First tooth. The germ of the first tooth appears in the 5th month of uterine life. Mineralization begins in the 6th month of life, when cuttings appear. By the 9th month, a small part of the crown is mineralized, by the end of the first year - about 1/3 of the crown, by the 2nd year - about half of it. By the end of the 3rd year, signs of cervical formation appear. By the 5th year, the entire crown and neck are already formed. By the 6th year, root growth begins. At the age of 7, the tooth erupts. By the 10th year, root growth ends; by this time the apex is already fully formed.
Second tooth. The tooth germ appears in the 5th month of uterine life. Dental shards appear in the 9th month of life. By the end of the first year of life, approximately 1/4 of the crown is mineralized, by the 3rd year - about half of it. By the 4th year, signs of cervical formations appear. By the end of the 6th year, the entire crown and neck are formed and root formation begins. At the age of 8 the tooth erupts. By the 12th year, root growth ends, the tip of which is fully formed by this time. Sometimes the completion of the formation of the root of the second tooth is somewhat delayed, ending by the 13th year.
Third tooth. The rudiment appears in the 5th month of the embryonic period, the dental shard - in the 6th month of life. At the 9th month, the top of the crown is mineralized, by the end of the first year - about 1/4 of the crown, by the 4th year - 2/3 of it. By the 7th year, the entire crown has already been formed and the neck of the tooth begins to develop; By the 8th year, the neck of the tooth is formed and root formation begins. By the 12th year, the formation of the root ends, except for its apex, which is finally formed by the 14th year, when the apical opening narrows to its minimum size. The end of root growth is sometimes delayed up to 16 years.
Fourth tooth. The rudiment appears towards the end of the embryonic period. In the 2nd year of life, the fourth tooth sac appears. At two and a half years old, shards appear. By the 4th year, about 1/4 of the crown is mineralized. By the 7th year, crown development ends and root growth begins. By the 13th year, root formation ends, the apical opening narrows to its minimum size. The end of root growth is sometimes delayed until the age of 14.
Fifth tooth. The tooth germ appears at the end of the first year of life or 3-4 months later. At 3 years old, shards appear. By the 5th year, about 1/4 of the crown is mineralized, by the 6th year - about 1/3 of the tooth. By the 8th year, the crown is already fully formed, and the neck of the tooth is outlined. By the 9th year, the neck is fully developed and root growth begins. At the age of 10, the tooth erupts. At the age of 14, root formation ends, and the apical foramen takes on its normal size. Root growth is sometimes completed at 15 years.
Seventh tooth. The tooth germ appears at the end of the first year. By the age of 3, shards appear. At the 4th year, about 1/4 of the crown is mineralized, by the 6th year - about 1/2. By the 8th year, the crown is already fully formed and the neck of the tooth is developing. By the 9th year, the development of the neck is completely completed and root growth begins. At 10-12 years of age, the tooth erupts. By the 12th year, the entire crown of 1/2 of the root is mineralized. At 14-17 years of age, root formation ends and the apical openings take on their normal size.
Eighth tooth. The rudiment appears at 4-5 years. In the 8th year, shards appear; in the 12th year, only the crown of the tooth is mineralized.
The first molar takes the longest to develop. By the time the child is born, mineralization of the crown of this tooth usually begins, the shards of which appear during uterine life - in the last month of pregnancy. Rarely does a newborn not experience the onset of mineralization of this tooth. The sixth tooth erupts at 6 years, rarely at 4-5 years, more often at 7 years. The growth of the roots of this tooth ends, as we have already indicated, often at 12 years of age. Using our x-ray material, we observed many cases where the apexes of the roots of the sixth tooth were not yet fully formed long after the normal period of growth of the roots of this tooth. We made the same observations in relation to the seventh, fifth, and fourth teeth, in which the roots turn out to be fully formed by normal dates. These observations are confirmed by the discovery of unformed apices on extracted teeth.
On average, the development of the root of each tooth lasts at least 4 years. For example, the development of the root of the sixth tooth lasts on average 5 years, the seventh - 5-6 years, the canine - at least 5 years, the root of the lateral incisor - at least 4 years, the first incisor - about 4 years. The roots of small molars develop on average over 4 years. This period should be considered from the moment of tooth eruption until the time of complete formation of the apical foramen. The formation of the root of the first small molar ends at the age of 12 to 14 years, the second small molar - at approximately 14-15 years. A canine that erupts at 11-12 years of age sometimes does not have a fully formed root until 15-16 years of age.
The intensity of mineralization depends on the nature of nutrition and the general condition of the body. For the most part, mineralization of certain areas ends within normal periods. Sometimes it ends prematurely, often it is delayed.
Lecture
for 2nd year students of the Faculty of Dentistry on the topic:
"Anatomy-morphological, histological and radiological features of the dentofacial system in children at different age periods."


Periods of development and formation of temporary teeth
1st – intrauterine development
formation of tooth buds
histogenesis
2nd – teething
4th - stabilization
5th - root resorption

Periods of development and formation of permanent teeth
1st – intrauterine development
formation of tooth buds
differentiation of tooth germs
histogenesis
mineralization of hard tooth tissues
2nd – teething
3rd – formation and growth of roots and periodontium
4th - stabilization

Stages of root formation
Unformed tip stage
Unclosed apex stage
Stage of formed root and periodontium
Stage of periodontal formation

Stages of root formation
Bell stage (stage of root growth in length)





^ TYPES OF TEETH ROOT RESORPTION
Physiological resorption
Pathological resorption
Idiopathic resorption

Uniform resorption of all roots




^ PULP STRUCTURE
- Odontoblasts (ODB) cells, specific to the pulp, form dentin and provide its trophism.
Neighboring ODB are connected by intercellular connections, thanks to which the ODB layer is able to perform a barrier function, regulating the movement of molecules and ions between the pulp and predentin.
- Fibroblasts (PB) are the most numerous pulp cells in young people.
The function of FB is the production and maintenance of the necessary composition of the intercellular substance of connective tissue, the absorption and digestion of the components of the intercellular substance. Signs of high activity are characteristic of FB in the teeth of young people.


Lymphocytes
- Lymphocytes (Lc) - in small quantities, during inflammation their content increases sharply. Pulp cells belong to different subpopulations of T cells; cytotoxic suppressors predominate. B cells are not normally found, but during inflammation they become numerous. These cells actively synthesize immunoglobulins (mainly IgG) and provide humoral immune responses.
- Mast cells (Tc) - located perivascularly, characterized by the presence in the cytoplasm of large granules containing biologically active substances: heparin, histamine, eosinophil chemotactic factor and leukotriene C. On the outer membrane of the Tc there are receptors for IgE. MC degranulation promotes increased vascular permeability and reduction of smooth myocytes.


For baby teeth:
1st period – development of the functional activity of the pulp (tooth root formation);
2nd period – functional maturity of the pulp (stabilization of the formed tooth root);
3rd period – fading of the functional properties of the pulp (resorption of the tooth root).

Pulp of primary teeth
Higher cell content, especially in the central layer, with fewer collagen fibers.
The volume of the pulp chamber and the pulp itself is larger in primary teeth.
Thinner layers of enamel and dentin - the pulp is closer to the external environment than in permanent teeth.
The differences between the structure of the coronal and root pulp are unclear.

The period of development of the functional activity of the pulp (the period of tooth root formation).
The cavity of an erupted milk tooth does not have a constant shape and size due to the ongoing formation of roots.
In the peripheral layer, the ODB are located in 3-4 rows. In the central layer there are numerous poorly differentiated cells.
The main substance of the pulp is dominated by acidic MPS and hyaluronic acid. Under the ODB layer are precollagen and reticulin fibers. Collagen fibers are almost absent.
In the first years of tooth growth, when the pulp morphologically resembles embryonic tissue, plastic properties pulps are especially pronounced.

The period of extinction of the functional properties of the pulp is the period of resorption of tooth roots.
The pulp undergoes involutive changes: the cellular composition decreases and the amount of collagen fibers, intermediate substance and tissue fluid increases.
Reticular or fatty degeneration and fibrosis occur in the pulp.
Some of the blood vessels are reduced, their walls thicken, congestive hyperemia occurs, and the nerve elements of the pulp change.
The vitality of the pulp is maintained thanks to the resorption organ, from where nutrients are delivered.

For permanent teeth:
1st period – formation of functional maturity of the pulp (formation of the tooth root);
2nd period – the onset of functional maturity (fully formed tooth roots without signs of aging);
3rd period – decrease in the functional activity of the pulp (fully formed roots with signs of tooth aging).

^ PULP OF PERMANENT TEETH.
The period of formation of the functional maturity of the pulp is the period of formation of the tooth root.
Predentine in teeth with unformed roots is represented by a wide strip of equal thickness.
The ODB layer in teeth with developing roots is massive and includes 8-12 rows of cells located compactly. The number of cell rows depends on the function - there are more of them in places of intense dentinogenesis.
The pododontoblastic layer is represented by the TC, FB, preODB, and MK of the pulp.
Reticulin fibers are represented mainly by precollagen fibers, turning into collagen fibers.
Thus, the pulp of teeth with unformed roots can be characterized as unformed maturing connective tissue.

The period of functional maturity of the pulp (the period of a fully formed tooth root).
The ODB layer is compact. Intensive dentin formation continues until the onset of signs of tooth aging.
In the coronal pulp, secondary dentin is provided with tubules, without a radial direction. In the root pulp, ODB produces amorphous dentin, weakly canalized.
After the formation of the apical foramen, the coronal pulp is rich in intermediate substance, in which well-developed fibrillar structures are immersed. The pulp contains a sufficient amount of energy material - glycogen, acidic and neutral MPS, providing normal processes fiber formation, as well as RNA and DNA involved in protein metabolism. The pulp during this period is well supplied with blood, its functions of dentin formation, protection, and trophism are clearly expressed. The structure of the pulp of a fully formed tooth corresponds to mature connective tissue with established high physiological activity.

Mineralization of the crowns of the lateral teeth begins from the tops of the cusps, and of the incisors - from the cutting edge, and on the radiograph they look like pinpoint foci of calcification, their number varies. Thus, in the incisors there are usually three centers of calcification, in the canines - four, in the molars and premolars there are as many of them as there are tubercles on the chewing surface.
Mineralization extends down to the cervical region, and on the lateral teeth a ring, “cap” or “shard” stage is distinguished.
Fig. 6.1-4 Stages of mineralization of the follicle of a permanent molar.
On the incisors, the contours of a mineralized crown of different sizes are determined. In an infant, radiographs of the jaws reveal mineralization of 1/6 of the crowns of the central incisors, approximately 2/3 of the crowns of the lateral incisors, and sometimes calcification in the area of the canine apex, and noticeable calcification in the area of the cusps of primary molars. Sometimes areas of calcification are visible in the area of the cusps of the first permanent molar and the cutting edge of the incisor.
It has been noted that teething occurs a little earlier in girls than in boys. However, there are individual deviations from the average eruption norms. Even fluctuations within 6 months are considered normal. Rickets, chronic dyspeptic disorders, acute infections, endocrine diseases, nutritional disorders, hypovitaminosis can affect the timing of mineralization and teething. In such cases, x-ray examination allows us to determine the presence or absence of rudiments and assess the degree of their formation, taking into account age.
Mineralization of permanent dentition teeth begins with the first molars at 9 months intrauterine development. The timing of complete mineralization of the crowns and roots of temporary and permanent teeth is presented in Table 1.
Terms of mineralization of crowns and roots of temporary and permanent teeth
Radiologically, there are 5 stages of development of the tooth root and periodontium:
I - stage of root growth in length;
II - stage of unformed apex;
III - stage of unclosed apex;
IV - stage of unformed periodontium;
V - stage of complete completion of root and periodontal formation.
The X-ray picture of the unformed apex of the tooth root and the tissues surrounding it is as follows: the walls of the root are parallel, their width gradually decreases, ending in points. The root canal has a smaller width in the area adjacent to the tooth cavity, and a larger width at the developing apical foramen, which gives it a funnel-shaped or bell-like appearance. The periodontal gap has the same width along the entire length of the root; at the root apex it merges with the growth zone; the apical foramen is very wide.
At the stage of the open apex, the root walls are characterized by greater wall thickness; at the root apex they are not completely closed. Therefore, the radiograph clearly shows the projection of the apical foramen, which is usually not distinguished in teeth with a formed root. The root canal is wide, but with a smaller diameter at the apex than at the neck of the tooth. The periodontal gap also becomes visible in the area of the root apex, where it is wider than around other parts of the root. The wider periodontal gap remains for some time, and after the root apex completes its development, it closes.

An expanded periodontal gap in the area of the lower permanent central incisors is observed up to 11 years; in the area of lateral incisors and first molars - up to 11 years; fangs - up to 17 years. In older age, the periodontal fissure normally has a uniform width along its entire length, and the apical foramen is not projected. A change in the width of the periodontal fissure towards decreasing or increasing indicates the presence pathological process.
Fig 7.1 Fig 7.2 Fig 7.3.
Rice. 7.1-3 Stages of tooth root formation.
7.1 stage of unformed apex (bell);
7.2 stage of unclosed apex;
7.3 stage of complete completion of root formation
During the period of mixed dentition, it is radiologically determined displacement of the rudiments of permanent teeth to the alveolar process after completion of the mineralization process of the crown. It takes approximately 5 years from the end of crown formation to the complete eruption of permanent teeth. Eruption is preceded by physiological resorption of the roots of temporary teeth.
Along with resorption of the roots of temporary teeth in bone tissue reparative processes occur in the jaws; their combination ensures the presence of bone tissue around the resorbing roots.
Depending on the characteristics of resorption of the roots of temporary teeth
T. F. Vinogradova distinguishes three types of resorption:
Physiological, pathological and idiopathic. Physiological resorption occurs in intact teeth and teeth that were treated for caries and pulpitis not complicated by periodontitis. Pathological resorption occurs with periodontitis, periostitis, osteomyelitis, cysts, and tumor processes.
Depending on the location, three types of physiological resorption are distinguished:
1. Uniform resorption of all roots.
2. Resorption of one of the roots predominates, the so-called uneven type of resorption. More often, this type of resorption begins in the distal root of the lower and distal buccal roots of the upper molars. Uneven resorption can also be observed in single-rooted teeth.
3. Resorption predominates in the bifurcation area with preservation of the roots. This type of resorption can lead to communication with the coronal part of the pulp.
In single-rooted teeth, uniform resorption is more often observed, sometimes uneven - mainly on the lingual side of the root in the incisors and in the medial parts of the root - in the canines.

8.1 8.2 8.3
Rice. Types of root resorption according to T.F. Vinogradova.
8.1. Uniform resorption of all roots 8.2. Resorption of one of the roots 8.3. Resorption in the area of bifurcation
Physiological resorption develops unevenly, but covers the entire surface of the roots. In this case, the inner surface of the roots, located closer to the permanent tooth germ, is resorbed faster. In the later stages of physiological resorption, the dental pulp takes part in the process, carrying out the resorption of dentin from the side of the tooth cavity. The source of osteoclasts is the pulp cells.
Along with physiological, under the influence of a number of reasons, it can develop pathological root resorption(resorption as a result chronic inflammation, idiopathic resorption, resorption as a result of neoplasms).
Most often it occurs as a result of chronic inflammation in the periodontium of temporary teeth.
Pathological resorption of the roots of temporary teeth is carried out by multinucleated giant cells foreign bodies(A.V. Rusakov) and cells of the inflammatory infiltrate. The processes of bone formation are minimal and lag behind resorption. In this regard, with pathological resorption, the leading radiological sign is the destruction and absence of bone tissue between the roots of temporary teeth or around them. Pathological resorption does not obey the laws of physiological resorption. Natural periodontal tissue during this period is replaced by granulation tissue of the inflammatory infiltrate. Root resorption occurs through small, deep lacunae, which are filled with inflammatory cells. In the tissue of the inflammatory infiltrate there are often epithelial strands that occupy a large space and can grow throughout the entire thickness of the tissue and grow into the root canals. As the pathological process progresses, the roots of temporary teeth and the follicles of permanent teeth become separated, while during physiological resorption they come closer together. With pathological resorption, resorption of the still unformed roots of temporary teeth, roots separated from the follicle of a permanent tooth and the roots of adjacent teeth may occur.
The process of pathological resorption can spread to the follicles of permanent teeth, causing premature resorption of the bone shell of the follicle and eruption of the permanent tooth.
On radiographs during the period of mixed dentition, the teeth and rudiments are located in three rows:
in the dental arch - temporary teeth; below are the rudiments of permanent teeth, which are located on different stages formation; in the third row - the rudiments of the canines (on the upper jaw - under the lower orbital edge, and on the lower - above the cortical layer of the lower edge of the jaw).
Period of permanent occlusion. At the age of 12 - 13 years, all temporary teeth have been replaced and the dentition contains permanent teeth with varying degrees of root formation.
![]()

Fig.9.1-4 Development periods dental system child.
The enamel on the radiograph is presented in the form of an intense linear shadow that borders the dentin of the crown; it is better visible on the contact surfaces of the teeth. Dentin and cement are not differentiated on an x-ray.
Between the root and the cortical plate of the alveoli there is a narrow slit-like space - the periodontal fissure. Its width ranges from 0.10 to 0.25 mm.
On radiographs, temporary teeth differ from permanent teeth in the following ways:
1. The height of the crown and the length of the roots of temporary teeth are less.
2. The thickness of the hard tissues of temporary teeth is less than that of permanent teeth.
3. The roots of temporary teeth are short and less massive.
4. In primary teeth, the tooth cavity and root canals, especially in the front teeth, are much wider.
5. The roots of temporary molars extend from one another at a greater angle than in permanent ones.
6. Between the roots of temporary molars are the rudiments of permanent teeth.
The dental cavity on an x-ray is determined in the form of a rarefaction with clear contours against the background of the tooth crown, and the root canals - in the form of linear rarefaction with smooth and clear closing contours.
The teeth in the alveolar process are separated from each other by an interdental septum. In the primary dentition, the apices of the interalveolar septa have different outlines. The apex of the septum located between the central incisors of the upper jaw is bifurcated; between the incisors of the lower jaw, bifurcation of the interalveolar septum is rare. In the area of other anterior teeth, the apices of the interalveolar septa often have rounded, less often sharp, outlines.
In the third period of temporary occlusion (reduction), due to the appearance of physiological diastemas and three, the apices of the septa are flattened. In the area of primary molars, the apices of the interalveolar septa are always flat. The apices of the interalveolar septa are always projected near the enamel-cement border. The cortical plate of the septa is well expressed, but the looping of the spongy substance is unclear.
In the mixed dentition of erupting teeth in the lower jaw, the apices of the interalveolar septa are, as it were, cut towards the erupting tooth and are located at the level of the enamel-cementum border or near it. In this case, it seems that the periodontal fissure is widened at the neck and crown of the erupting tooth; compact record in upper section The septa on the side facing the erupting tooth are wider. The pattern of the spongy substance is unclear.
With the end of tooth eruption, the formation of the interalveolar septum ends and the peculiarities of its structure appear. This is expressed in the appearance of clear outlines of the apices of the septa and the pattern of the spongy substance.
In the anterior teeth, the apices of the interalveolar septa of the erupted teeth acquire sharp or rounded outlines with a clearly defined compact plate of the same width throughout. In most children and adolescents, the septum located between the central incisors, in addition to the two forms indicated above, may have a sort of forked apex; the length of the bifurcation sometimes reaches 2 mm. Flat tops with a distinct compact plate between the front teeth occur in cases where there is a diastema or trema between them. Due to the arched shape of the dental arch, only one interalveolar septum is often clearly visible on an x-ray. Therefore, to obtain a clear image of it in the area of the front teeth, it is necessary to direct the beam of rays to the septum that needs to be seen.
In the area of premolars and molars, the apices of the interalveolar septa are flat, less often rounded, and the septa themselves resemble a trapezoid. The compact lamina is projected as a clear and continuous light strip along the edge of the interalveolar septa. This line appears clearer and wider until the age of 13.
The pattern of the spongy substance of the interalveolar septa is different and depends on age. In the area of the front teeth it is often large-looped, less often - small-looped; in the area of premolars and molars, in most cases, enlargement of the loops of spongy substance in the direction from the top of the interalveolar septum to the apices of the roots is clearly expressed. The large-loop pattern is determined less often than the small-loop pattern. The large-loop pattern is more common in children under 11 years of age, and less common in older children.
Schemes for describing radiographs.
1).Overall rating radiographs:
a).full name patient, age, date of study;
b).research method (intraoral contact radiograph, orthopantomogram, etc.);
c).projection of the study (direct, right or left lateral axial);
d).area of study on intraoral radiographs (tooth number);
2).Study of the tooth:
a).location (offset, etc.);
b).coronal part (size, shape, contours, presence of a carious cavity, presence of filling material and the degree of filling of the carious cavity with it, the nature of the filling, its overhang, etc.);
c).root (degree of visualization, degree of resorption);
d).tooth cavity (whether it communicates with a carious cavity, the degree of obliteration and filling filling material root canals;
e).periodontal gap (width in mm, uniformity, absence in certain areas, etc.).
3).Study of the tissues surrounding the tooth:
a). compact plate of the socket (preserved, destroyed, compacted, thickened);
b).interdental (interalveolar) septa (preserved, degree of height reduction, complete destruction);
c).periapical region (absence or presence of foci of destruction in the form of clearing, their number, size, shape, contours, structure, rim of darkening, presence of foci of compaction in the form of darkening with the same characteristics);
d).condition of the cortical tissues of the jaws (thinning or thickening, bulging, destruction);
d).mandibular canal (degree of visualization, displacement, etc.);
e).alveolar processes (state of the contours of the marginal sections, bone structure, osteoporosis, osteosclerosis, sequestration, etc.) -
4).Study of the temporomandibular joint:
a).articular space (narrowed, widened, uneven, degree of visualization);
b).ratio articular surfaces(dislocation, subluxation);
c).endplates of the epiphyses (sclerosation, thinning, disappearance, cystic clearing, etc.);
d).head of the condylar process (size, shape, contours, mobility, structure);
e).neck of the condylar process (change in angle relative to the head, shortening, etc.);
f).articular tubercle (flattening, structure, etc.);
5. Study of soft tissues (increase, decrease, additional shadows or brightening);
6. Conclusion about the nature of the pathological process. IN in doubtful cases Recommendations on the further algorithm of radiological methods should be given.
Lesson topic: Teleradiography techniques.
1. Relevance of the topic: Theoretical knowledge and practical skills in analyzing teleroentgenograms using the basic methods of Schwartz and Downes will allow for differential diagnosis of gnathic and dentoalveolar forms of dentoalveolar anomalies.
Based on the knowledge gained, an understanding will be formed medical tactics treatment of certain dental anomalies, choice of treatment with or without removal of permanent teeth, the need to use additional surgical methods to optimize orthodontic treatment.
2. Learning objectives of the lesson: To train students in methods of analyzing teleroentgenograms and, based on systematization of the acquired knowledge, formulate conclusions for developing a further plan of treatment and preventive measures for eliminating dental anomalies.
3. Personal development goals. Teach students to have a polite attitude towards parents and children of different ages with anomalies of the dental system.
Formation of milk roottooth In the process of root formation, it is customary to distinguish two stages: I - unformed apex and II - unclosed apex. In stage I, the root walls are thin and run parallel to each other. The canal is wide, at the apex it further expands and passes into the growth zone, which is presented in the form of a focus of rarefaction of bone tissue, limited along the periphery by a clearly defined cortical plate. In stage II, there is non-closure of the apex of the root, which is completing its formation. At this stage, the canal walls are formed, rounded and come closer together at the apex, the canal narrows at the apical foramen, and there is no growth zone at the apex. In place of the growth zone, a slight expansion of the periodontal fissure remains, which persists for about a year after the end of the formation of the apex.
Anatomical features of the mo primary teeth. IN the clinic have
The significance of their following features. There are 20 teeth in the primary dentition; premolars are missing. The teeth of the first eruption are white, resembling skim milk. The shape of the crowns of baby teeth is in general similar to that of permanent teeth, but they are much smaller, the layer of hard tissue is thinner, and the dental cavity is larger. Root canals and apical foramina are wide during the period of formation and resorption. The border between the crown and the root is sharply expressed. A more reliable sign of differentiation is a protruding thickening of the enamel. (enamel roller) in the cervical area and less hardness of baby teeth. In addition to general characteristics, there are individual characteristics.
Incisors. Baby teeth have incisors that are more convex than permanent teeth. There are no grooves on the palatal surface. The signs of the angle are clearly expressed. The distal angle of the maxillary lateral incisor is more rounded than that of the central incisor. The ridge of enamel on the lateral incisor at the neck is less pronounced than at the central one. The roots of the central incisors of the upper jaw are widened, and their apices are often curved towards the labial side. The crowns of the central incisors of the lower jaw are smaller. Their roots are flat, with grooves on the medial and lateral sides.
Fangs. Crown milk canine The upper jaw is usually shorter than the permanent one and has convex surfaces. It is characterized by the presence of a sharp tooth on the cutting edge and pronounced tubercles on the palatal surface. The crown of the lower jaw canine is narrower than the upper canine. The tooth remains on it longer. The root of the fang is round in shape with a slightly curved apex.
First molars. The crown of the first molar of the maxilla is elongated in
in the medial-distal direction, there are two cusps on the chewing surface with a pronounced bucco-medial cusp. The palatal surface of the crown is more convex. There are two grooves on the buccal surface of the tooth, giving the impression of a ribbed surface. The first primary molar of the maxilla has three widely divergent roots. Their tops seem to be cut off, the apical openings are wide. The crown of the first primary molar of the mandible is elongated in the anteroposterior direction. The four cusps on the chewing surface are better defined than on other teeth. The enamel ridge in the neck area is well developed. The buccal surface is divided into two parts: medial - wide and distal - narrow. The first primary molar of the mandible has two strongly divergent roots. The medial root is longer and wider than the distal one.
Second molars. The second primary molars of the upper jaw are characterized by an oblique crown shape and a pronounced enamel fold located between the anterior lingual and posterior buccal cusps, as well as fusion of the posterior buccal root with the palatal root and the absence of a root sign. In the first primary molar of the upper jaw, this sign is well expressed. The second primary molars of the lower jaw are similar in shape and structure to the first permanent molars of the same jaw. There are 5 tubercles on the chewing surface of the crown: 3 of them are located along the buccal edge, and 2 are located along the lingual edge. The most pronounced tubercle is the anterior buccal one. The roots of these teeth are no different in shape from permanent ones, they only diverge more to the sides.
Resorption of milk roots teeth(see table 1.1). After 5 years, the change from primary to permanent bite begins. This is before
Table 1.2. Timing of formation and eruption of permanent teeth
enamel poplasia, it is necessary to know the periods of intramaxillary tooth formation. Timing and sequence play a role in recognizing edentulous lesions.
Big practical significance acquires knowledge of the timing of root growth and periodontal formation. The doctor is guided by these data when determining the indications for the use of various methods of treating pulpitis, orthodontic equipment, etc. When analyzing radiographs of permanent teeth, it is advisable to distinguish two stages in the process of formation of the apical parts of the root: I - unformed apex and II - unclosed apex.
In stage I, the root length reaches normal size, its walls are parallel and appear pointed in the region of the root apex. The root canal is wide and ends at the root apex with a socket. Perio-
the growth of the rudiments of permanent teeth and the physiological resorption of the roots of milk teeth, which look shortened and corroded, proceed. Resorption of the roots of baby teeth begins with the root to which the permanent tooth germ is closest. The rudiments of the permanent teeth of the anterior group are located at the lingual surface of the root of the primary teeth, and the rudiment of the canine is located much further from the alveolar edge of the jaw than the incisors. The rudiments of premolars are located between the roots of primary molars: on the lower jaw closer to the posterior root, and on the upper jaw closer to the posterior buccal root, therefore, in single-rooted primary teeth, resorption begins from the lingual surface of the root, and then covers the root from all sides . In primary molars, resorption begins from the inner surface of the roots, i.e. from the surface facing the interradicular septum, where the permanent tooth germ is located. When the roots are reabsorbed, the pulp of baby teeth is replaced by granulation tissue, which takes part in the resorption process. With significant replacement of the pulp by granulation tissue, resorption occurs additionally from the center. It ends when the permanent tooth erupts.
Normally, the processes of eruption and resorption are completely balanced, but sometimes this physiological process is accompanied by deviations. An acceleration or deceleration of the resorption process is observed. Accelerated resorption is most often observed in baby teeth with dead pulp, after chronic trauma, in the presence of a tumor, as a result of pressure exerted by neighboring teeth. Slow resorption is found in the absence of permanent tooth buds.
Resorption of the roots of primary teeth must be taken into account in the treatment of pulpitis, periodontitis, tooth extraction and orthodontic interventions. Treatment of teeth with resorbed roots has its own specifics and differs from the method of treating and filling formed baby teeth.
Terms of eruption of constants teeth(Table 1.2). Time of eruption of permanent teeth replacing milk teeth, with proper development child coincides with the time of loss of baby teeth. Usually, after the loss of a milk tooth, the eruption of a permanent tooth begins, part of the cutting edge or cusps of which are visible after the loss of a milk tooth. However, there are cases of some delay in the onset of permanent tooth eruption. The number of lost baby teeth usually slightly exceeds the number of erupted permanent teeth. The eruption of permanent teeth begins with the first molar at 6 years of age. At this time, 3 rows of teeth can be seen on the x-ray. The first row includes milk teeth standing in an arch, sometimes even the first permanent molar; the second row contains the rudiments of permanent teeth different phases development, in the third row are the canines of the upper jaw, localized under eye orbits, on the lower jaw - directly under the cortical layer of the lower edge of the jaw body.
By the age of 12-13, all baby teeth are replaced by permanent teeth. The permanent teeth remain in the bite with varying degrees root formation. To resolve issues related to recognizing the disease and choosing treatment tactics, the pediatric dentist should remember the main periods of development of permanent teeth. Yes, when differential diagnosis gi-
The dontal fissure is visible only along the lateral walls of the root; it is not defined in the apical region. The compact plate of the socket wall is clearly defined throughout the entire length of the root. This stage is observed at the age of 8 years for the central and lateral incisors of the upper jaw, at 6 years for the central incisors of the mandible, at 7-8 years for the lateral incisors of the mandible and at 8 years for the first molars of the mandible.
In stage II, the walls of the tooth root are formed, but in the area of the root apex they are not close enough, as a result of which a wide apical foramen is revealed on the radiograph. The root canal is wide, but its diameter in the apical region is smaller than in the cervical region. The periodontal gap is well defined. In the area of the apex the gap is wider than in other sections. The compact plate of the hole along its entire length is
the root zone is clearly expressed. This stage is observed at the age of 9-13 years for the central incisors of the upper jaw, at 9-12 years - for its lateral incisors, at 7-11 years - for the central ones, and at 8-11 years - for the lateral incisors of the lower jaw, and at 8 -10 years - for the first molars of the lower jaw. After the closure of the root apex, the periodontal fissure continues to remain widened for about a year, especially in the area of the root apex.
Thus, the completion of the formation of the roots of permanent teeth occurs between the ages of 10 and 15 years. The end of the formation of tooth roots is determined radiographically when the apical foramen is not revealed on the image and there are clear contours of the periodontium. The dentofacial apparatus reaches the highest differentiation by the age of 15-18 years. It should be remembered that there are significant differences between permanent teeth in children and adults, both anatomically and biologically. Anatomically, in children's permanent teeth, the dental cavity and pulp are much larger in volume with a correspondingly smaller amount of hard tissue, so strong exogenous irritations pose a great danger to the pulp.
1.2.4. Structural features of some organs and systems
Nervous system. The main functions of the nervous system - central, peripheral, autonomic, coordinated by the cerebral cortex, are the regulation of all physiological processes of the growing organism and its continuous adaptation to the changing conditions of the internal and environment. The nervous system is formed at the earliest stages of the embryonic stage of development.
vitiia (2-3rd week), and its intensive development is noted throughout the entire period of pregnancy. A child is born with a large, but morphologically and functionally immature brain, the further improvement and differentiation of which occurs under the influence of the external and internal environment until the age of 20-25.
Brain. The size and weight of the brain at birth are relatively large - about 400 g, which is %, total body weight (in an adult - at 40 ). By the age of 20, it increases 4-5 times. In a newborn, cortical cells, nerve centers, striatal body, pyramid paths underdeveloped. Gray and white matter are poorly differentiated. Myelination of individual cells and pathways ends at different times: intracranial nerves by 3-4 months, cranial nerves (with the exception of the vagus) - by the first year, pyramidal tracts - by 2-3 years.
Spinal cord by the time of birth it has a more complete structure; by 2 years it almost corresponds to the spinal cord of an adult and is functionally more perfect than the brain.
Peripheral nervous system in a newborn it is represented by rare, insufficiently myelinated and unevenly distributed bundles of nerve fibers, the myelination of which ends in the 2-4th year of life.
Autonomic nervous system already functions in a newborn. By the age of 3-4 years, central regulation of the activity of the respiratory and circulatory organs is established. In young children, sympathicotonia is physiological, giving way to vagotonia at the 3-4th year; then equilibrium of the two systems is established, and in puberty vegetative-vascular dysto-
nia against the background of hormonal changes.
By the time of birth, the peripheral sections of the analyzers - the sensory organs - are structurally formed, but they do not function sufficiently due to the immaturity of the cortical centers.
When assessing the higher nervous activity of a child and the correspondence of the development of the central nervous system to his age, it is necessary to remember the following: I) differentiation of nerve cells, myelination of pathways and nerve trunks occur in a certain sequence; 2) the formation of conditioned reflexes is possible only as a result of repeated repetition of irritation and its reinforcement (in early childhood- food dominant); 3) structural improvement of the cortex goes parallel to the development of function, and the latter, with proper education (directed development of positive and negative conditioned connections), can anticipate the formation of morphological substrates and contribute to it.
Clinically, insufficient development of the nervous system manifests itself in certain patterns. Young children are prone to more severe, generalized reactions in response to any impact: infection, intoxication, pain and mental trauma. Local specific signs of the disease are often smoothed out, and general symptoms come to the fore: fever, vomiting, diarrhea. A young child has difficulty identifying the painful area.
At an early age, a general somatic reaction to the disease prevails, which reduces the significance local manifestations in the maxillofacial area, which complicates timely diagnosis and delays the provision of specialized care
power to the child. It is especially important to remember this in case of acute inflammatory diseases of the maxillofacial area in newborns and children of the first years of life.
In children who have been subjected to rough manipulations that do not spare the psyche without adequate anesthesia and switching off consciousness (forcible treatment and tooth extraction, suffocation and agitation during induction of ether anesthesia, etc.), a disturbance in the psycho-emotional state of the child is much more often observed. a long period. In preparing such patients for the treatment of dental diseases, the participation of a clinical psychologist is necessary. Such a reaction of the child (as a feature of the central nervous system function) is one of the important factors that expands the indications for premedication measures and absolute readings to surgical and therapeutic treatment, as well as to perform many dental procedures under anesthesia.
The cardiovascular system. Bookmark the heart and large vessels occurs in the 3rd week of the embryonic phase. The brain and liver receive more oxygenated blood, and lower limbs- in less.
The heart of a newborn is relatively large, approximately 0.8 % body weight. The most intense increase in the mass and volume of the heart is observed in the first years of life and adolescence. However, during all periods of childhood, the increase in heart volume lags behind the growth of the body as a whole. In addition, the parts of the heart increase unevenly: up to 2 years, the atria increase most intensively, from 2 to 10 years - the entire heart, after 10 years - mainly the ventricles.
Coronary vessels up to 2 years of age are distributed according to the scattered type, from 2 to 6 years - according to the mixed type, after
w ji^i
--
nu adult, mainline, type. The lumen and thickness of the walls (due to the intima) of the main vessels increase, and the peripheral branches are reduced.
In the first 2 years of life, intensive growth and differentiation of the myocardium occurs: muscle fibers thicken 1.5 times, by 10 years its histological structure is similar to that of adults. The heart is innervated through superficial and deep plexuses formed by fibers vagus nerve and cervical sympathetic nodes. Until 3-4 years of age, cardiac activity is regulated mainly by the sympathetic nervous system, which partly explains the presence of physiological tachycardia in these children in the first years of life.
In newborns, the cardiovascular system is most developed. The heart rate of children is higher than that of adults, and blood pressure is lower. Blood volume in children ranges from 80 to 150 ml per 1 kg of food weight (in adults 60 ml/kg). The blood flow rate in younger ages is also approximately 2 times higher, in adults, most of the blood circulates in the central blood vessels internal organs, and the peripheral blood circulation is reduced, baroreceptors are poorly developed. Children are very sensitive to blood loss and orthostatic sensations. The loss of 50 ml of blood in a newborn corresponds to 600-1000 ml in an adult; therefore, even a small loss of blood in a young child should be fully compensated in terms of volume and quality.
Functions of the circulatory organs - delivery of oxygen and nutrients to all organs and organs; removal and excretion of carbon dioxide and other waste products are carried out in close interaction with the respiratory organs
niya, digestion and excretion under the regulating influence of the central nervous system, autonomic and endocrine systems. Growth, structural and functional improvement of the circulatory organs continue throughout the entire period of childhood and occur unevenly, with the non-simultaneous maturation of individual parts, and the intense metabolic processes occurring in the child place high demands on their activity.




