Accessory hepatic artery. Blood supply to the liver. Hepatic arteriovenous fistulas
All these vessels arise from the common hepatic artery. In practice, the following is done: they look for the convex arch of the hepatic artery in the hepatoduodenal ligament and, certainly sparing this vessel, tie off all the lateral branches extending from it. All these branches go to the stomach, duodenum and pancreas, that is, parts that still have to be resected.
D) The splenic artery is dissected above the upper edge of the pancreas not far from its branch from the celiac artery, not reaching the place where it gives branches to the pancreas. It is necessary, firstly, to ensure that the left gastric artery, which also leaves the celiac artery, remains completely intact, since after the operation the remaining stump of the stomach is supplied with blood by this single vessel. The stump of the stomach will probably become necrotic if this vessel is also ligated. Secondly, when ligating the splenic artery, one must also be careful: the common hepatic artery, which arises from the celiac artery, cannot be ligated together with it.
D) The splenic vein is dissected on the posterior surface of the pancreas. It has already been mentioned above that the splenic vein, which receives numerous small branches from the pancreas and is closely adjacent to the posterior surface of the gland, can be easily elevated from the posterior abdominal wall, from which it does not receive vascular branches. As soon as the spleen with the tail and body of the pancreas is raised from the depths, then - if you follow the splenic vein on the posterior surface of the pancreas to the midline,
Data-lazy-type="image" data-src="operations%20on%20small%20intestine%20(495k)++.files/image010.jpg" width="468" height="445" class="lazy lazy -hidden ">
It becomes visible that approximately on the left edge of the spine, passing up and to the right, the inferior mesenteric vein flows into it.
With further dissection, it is necessary to get into the layer between these large veins and the pancreas, since these veins and their continuation, the superior mesenteric and portal veins, must remain intact. On the posterior surface of the pancreas, the splenic vein distal to the mouth of the inferior mesenteric vein is ligated in two places, at least 1 cm apart from each other, and dissected between them. The distal segment of the vein is left on the pancreas, the proximal segment is separated from the posterior surface of the pancreas so that it can remain with the inferior mesenteric vein on the posterior abdominal wall.
The common hepatic artery can be ligated because adequate collateral circulation is possible through the gastric and gastroepiploic arteries.
The proper hepatic artery can be ligated for a long time only proximal to the branch of the right gastric artery.
Venous blood supply to the liver carried out by the portal vein (v. portae), which is formed behind the pancreas at the confluence of the superior mesenteric vein with the splenic vein and carries blood from the stomach and intestines (Fig. 11-49). It goes through the oven
nocturnal duodenal ligament (lig. hepato-duodenal), located to the left of the common bile duct (ductus choledochus), but to the right of the proper hepatic artery (a. hepatica propria), and is divided into the right and left lobar portal veins (vv. portae lobares dextra et sinistra), which enter the portal of the liver. The branches of these veins end in the venous sinuses of the liver. The portal vein can be clamped during surgery for no longer than 30 minutes.
Venous drainage from the liver (Fig. 11-50) carried out into the inferior vena cava (v. cava inferior), which leaves a groove in the extraperitoneal field of the liver, where three hepatic veins flow into it (vv. hepaticae). When the hepatic veins are damaged, intense venous bleeding is observed, which cannot be stopped by squeezing the hepatic-duodenal ligament.

Rice. 11-50. Diagram of blood circulation in the liver. 1 - hepatic vein, 2 - hepatic duct, 3 - portal vein, 4 - proper hepatic artery.
Lymphatic drainage
Lymphatic vessels leaving the liver
neither together with the vascular-secretory pedicle, pour into the hepatic lymph nodes (nodi lymphatici hepatici), located in the hepatoduodenal ligament, and further into the celiac lymph nodes (nodi lymphatici coeliaci).
Lymphatic drainage from the diaphragmatic surface
the liver is possible in the posterior mediastinal
The lymph nodes (nodi lymphatici medio-stinales posteriores).Innervation (Fig. 11-51)
Branches of the sympathetic hepatic plexus (plexus hepaticus), located on the portal vein and proper hepatic artery.
Hepatic branches of the vagus nerves (rami
hepatici pp. vagi), approaching the gate of the liver.
Branches of the right phrenic nerve
(n. phrenicus dexter) from the bottom side
the top of the diaphragm approaches the bottom
vena cava and then go to the gate
liver.
EXTRAHEPATIC BILIAL TRACT
Extrahepatic bile ducts ways They begin with the right and left hepatic ducts emerging from the porta hepatis, which lie between the layers of the hepatoduodenal ligament and, merging, form the common hepatic duct (Fig. 11-52).
Left hepatic duct (ductus hepaticus
sinister) collects bile from the left and quadrate lobes, as well as the left half of the caudate lobe of the liver.
Right hepatic duct (ductus hepaticus
dexter) collects bile from the right lobe and the right half of the caudate lobe of the liver.
Common hepatic duct (ductus hepaticus
communis) has a length of 2-4 cm and stretches to
fusion with the cystic duct.
Cystic duct(ductus cysticus) located between the layers of the upper part of the hepatoduodenal ligament and connects the gallbladder with the common hepatic duct to form the common bile duct. The length of the cystic duct varies, but on average is 1-2 cm. It connects with the common hepatic duct at a more or less acute angle and has a spiral fold on the mucous membrane (plica spiralis).
Gallbladder (vesica felled) located in the fossa of the same name on the visceral surface of the liver and is projected at the intersection of the right costal arch with the lateral edge of the rectus abdominis muscle. Its length is 6-10 cm, width 3.5-4.5 cm, volume 30-50 ml. The gallbladder consists of a fundus (fundus), body (corpus) And
 |
| 6 7 |
Rice. 11-51 Diagram of the zone of irradiation of pain in diseases of the liver and biliary tract (a) and innervation of the liver (b). 1 - duodenum, 2 - common bile duct, 3 - gallbladder, 4 - liver, 5 - great splanchnic nerve, 6 - phrenic nerve, 7 - spinal ganglion, 8 - seventh-tenth thoracic nodes of the sympathetic trunk, 9 - vagus nerve , 10 - sensory fibers of the greater splanchnic nerve, 11 - sympathetic fibers of the greater splanchnic nerve, 12 - proper hepatic artery, 13 - celiac trunk, 14 - common hepatic artery, 15 - gastroduodenal artery. (From: Netter F.H.
cervix (collum) having an extension - a pocket of the neck of the gallbladder (recessus colli vesicae felleae), or pocket Hartmann, and passing into the cystic duct. The gallbladder most often lies mesoperitoneally and is covered by peritoneum from below, but sometimes an intraperitoneal position is observed (with the formation of a mesentery), and extremely rarely it can be covered by liver parenchyma on all sides and may not have peritoneal cover.
Common bile duct(ductus choledochus) has a length of 8-10 cm and a diameter of up to 1 cm.
Parts of the common bile duct Supraduodenal part (pars supraduodenalis) lies in the hepatoduodenal ligament (lig. hepatoduodenale) together with the portal vein (v. portae) and the own hepatic artery (a. hepatica propria). The common bile duct is located on the right in the pre-
affairs of the free edge of the hepatic-duodenal ligament, the proper hepatic artery is located in the hepatic-duodenal ligament on the left, and the portal vein is located between the proper hepatic artery and the common bile duct and somewhat behind them (Fig. 11-53).
Retroduodenal part (pars retroduodenalis) passes behind the upper part of the duodenum.
Pancreas (pars pancreatica) passes behind the head or through the head of the pancreas, has a sphincter (sphincter ductus choledochi) and merges with the pancreatic duct (ductus pancreaticus). The following options for connecting the common bile duct and the pancreatic duct are possible (Fig. 11-54):

Rice. 11-52. Extrahepatic biliary tract. 1 -
right and left hepatic ducts, 2 - common hepatic duct, 3 - cystic duct, 4 - common bile duct, 5 - pancreatic duct, 6 - accessory pancreatic duct, 7 - hepatopancreatic ampulla, 8 - descending part of the duodenum intestines, 9 - bottom of the gallbladder, 10 - body of the gallbladder, 11 - neck of the gallbladder, 12 - pocket of the neck of the gallbladder (Hartmann).(From: Moore K. L.

Rice. 11-53. Formations occurring in the hepatoduodenal ligament. 1 - bile duct (ductus choledochus), 2 - portal vein (v. portae), 3 - own hepatic artery (a. hepatica propria), 4 - common hepatic duct (ductus hepaticus communis), 5 - right hepatic artery (a. hepatica dextra), 6 - left hepatic artery (a. hepatica sinistra).
♦ the common bile duct and the pancreatic duct merge at the head of the pancreas;
♦ the common bile duct and the pancreatic duct merge in the wall of the duodenum;
♦ The common bile duct and the pancreatic duct open into the duodenum at separate orifices.
Hepatic-pancreatic ampoule(ampulla hepatopancreatica) is formed in approximately 65% of cases and is formed by the fusion of the common bile duct and the pancreatic duct (Fig. 11-55). It pierces the wall of the descending part of the duodenum in an oblique direction at a distance of 3-8 cm from the pylorus, opens on the large duodenal (Vaterov) papilla (papilla duodeni major) and has the same sphincter (sphincter ampullae hepatopancreaticae; sphincter of the major duodenal papilla, sphincter Oddie).
Blood supply, innervation, blood and lymph drainage
Blood supply
The common hepatic and supraduodenal part of the common bile duct are supplied with blood by the branches of the proper and right hepatic arteries (a. hepatica propria et a. hepatica dextra)(rice. 11-56).
The retroduodenal and pancreatic parts of the common bile duct are supplied with blood by branches of the posterior superior pancreaticoduodenal artery (a. pancreaticoduodenalis superior posterior).
The gallbladder is supplied with blood by the cystic vesicle
artery (a. cystica), arising most often from the right hepatic artery (a. hepatica dextra). Cystic artery, common hepatic duct (ductus hepaticus communis) and cystic duct (ductus cysticus) form a triangle Kahlo.
Bleeding from the gallbladder and the supraduodenal part of the common bile duct occurs along the gallbladder vein (v. cystica) into the portal vein (v. portae). Blood outflow from the retroduodenal and pancreatic parts of the common bile duct is carried out through the pancreaticoduodenal veins (vv. pancreaticoduodenalis) into the superior mesenteric vein (v. mesenterica superior).
Rice. 11-55. Sphincters of the common bile and pancreatic ducts, hepatopancreatic ampulla. 1 -
sphincter of the hepatopancreatic ampulla, 2 - sphincter of the common bile duct, 3 - sphincter of the pancreatic duct.
Lymphatic drainage from the gallbladder and extrahepatic bile ducts to the hepatic lymph nodes (nodi lymphatici hepatici), located in the hepatic-duodenal ligament, and further into the celiac lymph nodes (nodi lymphatici coeliaci).
Innervated extrahepatic bile ducts by branches of the vagus nerve (p. vagus), celiac (plexus coeliacus) and hepatic (plexus hepaticus) plexus.
The branches of the vagus nerve carry prenodal parasympathetic and sensory nerve fibers. Under the influence of the vagus nerve and as a result of the influence of cholecystokinin, the sphincter of the hepatopancreatic ampulla relaxes.
The celiac and hepatic plexuses receive
prenodal sympathetic and sensory nerve fibers as part of the greater splanchnic nerve (n. splanchnicus major). The branches of these plexuses contain post-nodal sympathetic nerve fibers and sensory fibers of the 6-8th thoracic segments of the spinal cord, as a result of which pain arising from pathology of the gallbladder and extrahepatic bile ducts is projected onto the right hypochondrium and epigastric region.
Atresia of the gallbladder and bile ducts
This is a fairly rare developmental defect, manifested by increasing jaundice and discolored stools from the moment of birth. Forms of atresia of the extrahepatic bile ducts (Fig. 11-57):
Atresia of the common bile duct;
Atresia of the common bile duct and gallbladder;
Atresia of the common bile duct and gallbladder and common hepatic duct;
Atresia of the gallbladder, common bile, common hepatic, right and left hepatic ducts.
PANCREAS
Pancreas (pancreas) develops from the ventral and dorsal primordia, which are protrusions of the epithelium of the embryonic intestine, merging with each other (Fig. 11-58).

Rice. 11-57. Forms of atresia of the extrahepatic bile ducts, a - atresia of the common bile duct, b - artesia of the common bile duct and gallbladder, c - artesia of the gallbladder, common bile duct and common hepatic duct, d - artesia of the gallbladder, common bile duct, common hepatic duct, right and left hepatic duct. (From: Doletsky S.Ya., Isakov I.F. Pediatric surgery. - M., 1970.)
From the dorsal primordium, most of the pancreatic parenchyma (body and tail) and the accessory duct of the pancreas are formed. .
From the ventral primordium, a smaller part of the pancreatic parenchyma (head) and the pancreatic duct are formed .
Disturbances in the fusion of the ventral and dorsal pancreatic buds can lead to changes in the shape of the pancreas and congenital stenosis of the duodenum (Fig. 11-59).
Options for changing the shape of the pancreas
The ring-shaped pancreas covers the descending part of the duodenum.
The claw-shaped head of the pancreas partially encloses the descending part of the duodenum.
 |
Rice. 11-58. Development of the pancreas and its ducts.
1 - common bile duct, 2 - ventral pancreatic bud, 3 - dorsal pancreatic bud, 4 - duodenum, 5 - accessory pancreatic duct, 6 - pancreatic duct. (From: Moore K. L. Clinically oriented Anatomy, 1992.)
The accessory lobule of the pancreas may be located in the submucosa of the duodenal wall. The pancreas is both an exocrine and an endocrine gland. Produced by islet cells Langer-hansa insulin and glucagon are involved

Rice. 11-59. Anomalies of the development of the pancreas.
a - ring-shaped pancreas, b - claw-shaped head of the pancreas, c - accessory lobe of the pancreas. (From: Bairov G.A., Doroshevsky Yu.L., Nemilova T.K. Atlas of operations in newborns. - P., 1984.)
in the regulation of carbohydrate metabolism, and the secretion of the exocrine pancreas contains enzymes necessary for the digestion of proteins, fats and carbohydrates.
Anatomical structure, location of the pancreas and its relationship to the peritoneum
The pancreas is projected onto the anterior abdominal wall within the epigastric and left hypochondrial regions. Its length is 15-20 cm, vertical size is about 4 cm with a thickness of about 2 cm, weight is 70-80 g (Fig. 11-60).
Parts of the pancreas
Head (caput) located to the right of the body
I lumbar vertebra and is surrounded above, right and below, respectively, by the upper, descending and lower horizontal parts of the duodenum. She has:
♦ front surface (facies anterior), covered with parietal peritoneum, to which the antral part of the stomach is adjacent above the mesentery of the transverse colon, and below - the loops of the small intestine;
♦ back surface (facies posterior), to which the right renal artery and vein, the common bile duct and the inferior vena cava are adjacent;
♦ top and bottom edges (margo superior et inferior);
♦ uncinate process (processus unci-natus), separated by pancreatic notch (incisura pancreatis).
At the border of the head and body, the neck of the pancreas is sometimes isolated.
Body (corpus) located in front of the body
I lumbar vertebra and has:
 |
Rice. 11-60. Pancreas and duodenum. 1 - head of the pancreas, 2 - descending part of the duodenum, 3 - superior flexure of the duodenum, 4 - upper part of the duodenum, 5 - body of the pancreas, 6 - groove of the splenic artery, 7 - tail of the pancreas, 8 - duodenum - jejunal flexure, 9 - jejunum, 10 - ascending part of the duodenum, 11 - uncinate process of the pancreas, 12 - lower horizontal part of the duodenum, 13 - lower flexure of the duodenum. (From: Kishsh-Sentagotai. Anatomical atlas of the human body. - Budapest, 1973. - T. II.)
♦ front surface (facies anterior), covered by the parietal peritoneum of the posterior wall of the omental bursa, to which the posterior wall of the stomach is adjacent;
♦ back surface (facies posterior), to which the aorta, splenic and superior mesenteric vein are adjacent;
♦ bottom surface (facies inferior), to which the duodenojejunal flexure is adjacent below (flexura duodeno-jejunalis);
♦ top, bottom and front edges (margo superior, inferior et anterior).
Tail (cauda) It has:
♦ front surface (facies anterior), To
which the fundus of the stomach is adjacent to;
♦ back surface (facies posterior), adjacent to the left kidney, its vessels and adrenal gland.
Pancreatic ducts(rice. 11-61). The pancreatic duct passes through the entire gland from the tail to the head. (ductus pancreaticus), which, connecting with the bile duct or separately from it, opens into the descending part of the duodenum on the major duodenal papilla (papilla duodeni major). Sometimes on the small duodenal papilla (papilla duodeni minor), located approximately 2 cm above the large one, the accessory pancreatic duct opens (ductus pancreaticus accessorius).
Peritoneum and ligaments(rice. 11-62)
 |
Rice. 11-62. Peritoneal cover of the pancreas. 1 - kidney, 2 - descending part of the duodenum, 3 - parietal peritoneum of the subhepatic bursa, 4 - pylorus, 5 - diaphragmatic-splenic ligament (crossed), 6 - parietal peritoneum of the posterior wall of the omental bursa, 7 - mesentery of the transverse colon (crossed) , 8 - duodenojejunal flexure, 9 - parietal peritoneum of the left longitudinal canal, 10 - jejunum, 11 - superior mesenteric artery, 12 - superior mesenteric vein, 13 - uncinate process, lined with the parietal peritoneum of the right mesenteric sinus. (From: Sinelnikov R.D. Atlas of human anatomy. - M., 1972. - T. II.)
| (a. gastroduodenalis), located between the head of the pancreas and the upper and descending parts of the duodenum. ♦ Anterior and posterior inferior pancreatoduodenal arteries (aa. pancreaticoduodenales, inferioris anterior et posterior) arise from the superior mesenteric artery (a. mesenterica superior), located between the head of the pancreas and the lower horizontal and descending parts of the duodenum. The body and tail of the pancreas are supplied by the pancreatic branches of the splenic artery (rr. pancreatici a. lienalis). The blood outflow of the pancreas is carried out through the veins of the same name, flowing into the superior mesenteric and splenic veins (v. mesenterica superior et v. lienalis). Innervation (Fig. 11-64). Branches of the celiac muscle take part in the innervation of the pancreas (plexus coeliacus), hepatic (plexus hepaticus), splenic (plexus lienalis), intermesenteric (plexus intermesentericus) and renal (plexus renalis) plexuses entering the gland mainly along the vessels and carrying postnodal sympathetic nerve fibers and sensory fibers from the 7-11th thoracic segments of the spinal cord and branches of the right vagus nerve (p. vagus), carrying prenodal parasympathetic and sensory nerve fibers. Prenodal |
The mesentery of the transverse colon is attached along the lower edge of the body of the pancreas; on the right, the root of the mesentery passes in the middle of the head. The head and body of the pancreas are covered with peritoneum only in front, i.e. located retroperitoneally, the tail of the pancreas is located between the layers of the splenorenal ligament (lig. lienorenale) and lies intraperitoneally.
Gastropancreatic ligament (lig. gastro-pancreaticum)- transition of the peritoneum from the upper edge of the pancreas to the posterior surface of the body, cardia and fundus of the stomach; the left gastric artery runs along its edge (a. gastrica sinistra).
Pylorogastric ligament (lig. pylo-
ropancriaticum)- transition of the peritoneum from the upper edge of the body of the pancreas to the antrum of the stomach.
Blood supply (Fig. 11-63)
The head of the pancreas has in common
blood supply to the duodenum.
♦ Anterior and posterior superior pancreatoduodenal arteries (aa. pancreatico-duodenales superioris anterior et posterior) arise from the gastroduodenal artery
 |
Rice. 11-63. Blood supply to the pancreas and duodenum. 1 - celiac trunk (truncus coeliacus), 2- common hepatic artery (a. hepatica communis), 3 - gastroduodenal artery (a. gastroduodenalis), 4 - superior posterior pancreaticoduodenal artery (a. pancreaticoduodenalis superior posterior), 5 - superior anterior pancreaticoduodenal artery (a. pancreaticoduodenalis superior anterior), 6 - inferior posterior pancreaticoduodenal artery (a. pancreaticoduodenalis inferior posterior), 7 - inferior anterior pancreaticoduodenal artery (a. pancreaticoduodenalis inferior anterior), 8 - dorsal pancreatic artery (a. pancreatica dorsalis), 9 - artery of the tail of the pancreas (a. caudae pancreatis), 10 - splenic artery (a. lienalis), 11 - superior mesenteric artery (a. mesenterica superior), 12 - great pancreatic artery (a. pancreatica magna), 13 -inferior pancreatic artery a. pancreatica inferior).(From: Netter F.H. Atlas of human anatomy. - Basle, 1989.)
 |
sympathetic and sensory nerve fibers enter the plexuses as part of the large and small splanchnic nerves (pp. splanchnici majores et minoris).
SPLEEN
Spleen - an unpaired parenchymal organ located in the upper floor of the abdominal cavity deep in the left hypochondrium at the level of the IX-XI ribs along the mid-axillary line (Fig. 11-65). Its approximate size is 12x7x3 cm, weight is about 150 g. The spleen has diaphragmatic and visceral surfaces (facies diaphragmatica et visceralis), front and rear ends (extremitas anterior et posterior), gates (hilum lienis). The spleen is covered by peritoneum on all sides, with the exception of a small area of visceral surface in the hilum area.

Rice. 11-65. Skeletotopy of the spleen, a - low, b - high position of the spleen. (From: Shevkunenko V.N. A short course in operative surgery with topographic anatomy. - M., 1947.)
The rudiment of the spleen is located between the layers of the dorsal mesentery of the stomach, which, after turning the stomach and moving the spleen to the left hypochondrium on the left, limits the splenic recess of the omental bursa (recessus lienalis) and turns into the gastrosplenic and splenorenal ligaments.
Gastrosplenic ligament (lig. gastro-lienale) goes from the greater curvature of the stomach to the hilum of the spleen, contains the left gastroepiploic vessels (a. et v. gastroepiploicae sinistrae) and short gastric arteries and veins (a. et v. gastrici breves).
Splenorenal (diaphragmatic-splenic) ligament stretches from the lumbar part of the diaphragm, from the left kidney to the hilum of the spleen and contains the splenic artery and vein between its leaves (a. et v. lienalis) and the tail of the pancreas.
The phrenic-colic ligament plays an important role in fixing the spleen. (lig. phrenicocolicum), limiting the blind recess of the spleen (saccus caecus lienis), in which, like in a hammock, lies the spleen.
Blood supply, innervation, blood and lymph drainage
Supplies blood spleen artery of the same name (a. lienalis), which arises from the celiac trunk (truncus coeliacus), passes along the upper edge of the pancreas, giving off pancreatic branches for its blood supply (rr. pancreatici), along the splenorenal ligament (lig. lienorenale) approaches the hilum of the spleen and gives off the splenic branches (rr. lienalis). The terminal branch of the splenic artery is the left gastroepiploic artery (a. gastro-epiploica sinistra), exiting along the gastrosplenic ligament (lig. gastroliennale) to the greater curvature of the stomach (Fig. 11-66).
Bleeding from the spleen it is carried out along the vein of the same name (v. lienalis), which goes slightly below the artery of the same name and passes behind the pancreas, where it flows into the portal vein (v. portae).
Lymphatic vessels the spleens leave the parenchyma in the area of its hilum and enter the splenic lymph nodes , efferent vessels of which along the course of the splenic artery reach the celiac lymph nodes (nodi lymphatici coeliaci).
Innervate spleen branches of the splenic plexus (plexus lienalis), which is located on the splenic vessels and receives prenodal sympathetic and sensory nerve fibers of the large splanchnic nerve (n. splanchnicus major), as well as prenodal parasympathetic and sensory nerve fibers of the vagus nerve (p. vagus) through the celiac plexus (plexus coeliacus).
 |
Rice. 11-66. Blood supply to the spleen.
I - celiac trunk, 2 - aorta, 3 - left celioepiploic artery, 4 - short gastric branches, 5 - spleen, 6 - left gastric artery, 7 - adrenal gland, 8 - kidney, 9 - splenic branches, 10 - splenic vein , 11 - tail of the pancreas, 12 - splenic artery, 13 - duodenojejunal flexure. From: Forged V.V. Operative surgery and topographic anatomy. - M., 1985.)
SMALL INTESTINE
Below the pyloric opening (ostium pyloricum) small intestine begins (intestinum renue), in which the digestion of food coming from the stomach is completed, and selective absorption of digestion products into the blood and lymph occurs. Small intestine, starting with the descending part of the duodenum (pars descendens duodeni), located in the lower floor of the abdominal cavity (see Fig. 11-60).
Duodenum
The initial part of the small intestine is the duodenum (duodenum), curving like a horseshoe around the head of the pancreas. The duodenum is divided into upper, descending, lower horizontal and ascending parts.
Top part (pars superior) extends horizontally from the pyloric opening (ostium pyloricum) to the top bend (flexura duodeni
superior) at the level of the first lumbar vertebra (see Fig. 11-61).
♦ It is located in the upper floor of the abdominal cavity: intraperitoneal - in the initial part, where the hepatoduodenal ligament fits (lig. hepatoduodenale), being the right part of the lesser omentum (omentum minus), limiting the stuffing box (foramen epi-ploicum) anteriorly and containing the common bile duct (ductus choledochus), portal vein (v. portae) and the proper hepatic artery (a. hepatica propria)(see Fig. 11-53), mesoperitoneally - in the middle part and retroperitoneally - in the area of the upper bend.
♦ The upper part of the duodenum contacts:
On top with the gallbladder;
From below with the head of the pancreas;
Posteriorly with the body of the first lumbar vertebra
In front with the antrum of the stomach.
Descending part (pars descendens) coming ver
tickly from the upper to the lower bends,
(flexura duodeni superior et inferior) to the right of the spine at level L 1 -L ii.
♦ It is located retroperitoneally; the peritoneum, when passing from the right and above to the right kidney, forms the duodenal-renal ligament (lig. duodenorenale, BNA).
♦ On the mucous membrane of the posterior internal surface there are: small duodenal papilla (papillae duodeni minor), located about 6 cm from the pylorus, where the accessory pancreatic duct opens ; large duodenal (vaterov) papilla (papillae duodeni major), located at a distance of about 8 cm from the pylorus, where the hepatopancreatic ampulla opens (ampulla hepatopancreatica).
♦ The descending part of the duodenum contacts:
On the left with the head of the pancreas;
Posterior and right with the right kidney, right renal vein, inferior vena cava and ureter;
In front with the mesentery of the transverse colon and below its attachment with the loops of the small intestine.
Bottom horizontal part (pars horizontalis
inferior) comes from the bottom bend (flexura duodeni inferior) to the intersection with the superior mesenteric vessels at level Liii.
♦ It is located retroperitoneally, its anterior wall lifts the parietal peritoneum of the right mesenteric sinus of the lower floor of the abdominal cavity.
♦ The lower horizontal part of the duodenum contacts:
Above with the head of the pancreas;
Rising part (pars ascendens) comes from
intersections with the superior mesenteric
ships at level Liii to the left and up to two-
duodenojejunal flexure (flexura
duodenojejunalis), located at the level
Lii, and is fixed by the hanging connection
which duodenum (lig. sus-
pensorium duodeni).
♦ The duodenal suspensory ligament extends from the duodenum-jejunal flexure (flexura duodenojejunalis) to the right leg of the diaphragm, contains not only collagen, but also muscle fibers, called the muscle that suspends the duodenum (i.e. suspensorium duodeni), and, lifting the peritoneum, forms the superior duodenal fold (plica duodenalis superior), in which passes the inferior mesenteric vein (v. mesenterica inferior). This ligament is an important landmark when performing surgical interventions.
♦ The ascending part of the duodenum is located mesoperitoneally, it contacts:
From above with the lower surface of the body of the pancreas;
Posteriorly with the inferior vena cava and abdominal aorta;
In front and below with loops of the small intestine.
Blood supply duodenum by the vessels of the celiac trunk and superior mesenteric artery (see Fig. 11-63). Common hepatic artery (a. hepatica communis) arises from the celiac trunk (truncus coeliacus), goes to the right along the upper edge of the pancreas to the hepatoduodenal ligament, where it divides into the proper hepatic artery (a. hepatica propria) and the gastroduodenal artery (a. gastro-duodenalis).
The supraduodenal artery takes part in the blood supply to the upper part of the duodenum (a. supraduodenalis) and retroduodenal arteries (aa. retro-duodenales), originating most often from the gastroduodenal artery, but sometimes from the common hepatic or right gastric artery. The supraduodenal artery may be absent.
The upper half of the descending part of the duodenum is supplied by the duodenal branches of the anterior and posterior superior pancreaticoduodenal arteries (rr. duodenales aa. pancreaticoduodenales superiores anterior et posterior), originating from the gastroduodenal artery.
The lower half of the descending, horizontal and ascending parts of the duodenum
The colon is supplied with blood by the duodenal branches of the anterior and posterior inferior pancreatoduodenal arteries (rr. duodenales aa. pancreaticoduodenales inferiores anterior et posterior), arising from the superior mesenteric artery (a. mesenterica superior).
Anterior and posterior superior pancreatoduodenal
nal arteries at the level of the middle lower part
walking part of the duodenum
anastomose with the lower ones of the same name
vessels.
Bleeding carried out through the veins of the same name into the portal vein system.
Lymphatic drainage from the duodenum is carried out to the upper and lower pancreatoduodenal lymph nodes (nodi lymphatici pancreaticoduodenalis superiores et inferiores) and further to the celiac lymph nodes (nodi lymphatici coeliaci).
Innervate duodenum branches of the vagus nerves (pp. vagi), carrying parasympathetic and sensory fibers through the celiac plexus (plexus coeliacus), in the formation of which the large splanchnic nerves also take part (pp. splan-chnici majores), carrying sympathetic and sensory fibers from segments Th 7 - 9 of the spinal cord, as a result of which, in pathology of the duodenum, pain is noted in the epigastric region (see Fig.
Aneurysms of the visceral branches of the aorta are a rare pathology, the incidence of which, according to routine autopsies and non-invasive diagnostic methods, does not exceed 0.1-2%. The first mention of an aneurysm of the hepatic artery was found by J. Wilson in 1809, in the autopsy report of a 50-year-old priest who died from a rupture of the “cavity associated with the left hepatic artery” (cited by Guida P.M. and Moore S.W.). In 1847, E. Crisp, studying descriptions of 591 cases of aneurysms of the visceral branches, did not find a single case of hepatic artery aneurysm among them. In 1891, Hale White first described a triad of clinical signs accompanying the disease, which included pain in the right upper quadrant of the abdomen, gastrointestinal bleeding and jaundice of the skin, which are still used to this day for the primary diagnosis of this pathology. By 1895, 21 cases of hepatic artery aneurysms had been reported, none of which were diagnosed antemortem and each of which resulted in the death of the patient. The first experience of successful treatment has been known since 1903, when H. Kehr first performed ligation of a hepatic artery aneurysm with a breakthrough into the gallbladder. In 1943, G. Gordon Taylor first used the aneurysmography technique. Thus, by 1954, 100 clinical observations of hepatic artery aneurysm were known, but in only two cases the diagnosis was made before surgery.
Hepatic artery aneurysm is a rare condition that is life-threatening if not diagnosed and treated promptly. Due to the wide incorporation of high-tech methods of diagnosis in medical practice, it is now possible to diagnose patients early, provide care and, as a result, increase the survival rate. Based on the review of articles published in foreign medical journals, authors highlight the role of radiological methods in the diagnosis of this pathology and present a case report showing their application. The present clinical case demonstrates the possibilities of diagnosis and treatment, as well as difficulties caused primarily by rarity of diseases.
Morphology and etiopathogenesis.
An aneurysm should be understood as a local expansion of the diameter of a vessel by 1.5 times compared to its non-expanded area. Depending on the mechanism of aneurysm formation, they are divided into true and false. True aneurysms develop when there are abnormalities in the vessel wall, resulting in expansion and thinning of all three layers. At the beginning of the last century, it was believed that the main etiological factor leading to the formation of true aneurysms is fungal infection, but currently a large role is given to atherosclerotic changes in the walls, especially in the presence of such risk factors as long-term hypertension, dyslipidemia, smoking, etc. Thus, in the analysis of 300 publications F.T. Curran and S.A. Taylor note that the incidence of atherosclerotic changes, both primary and secondary, is up to 32%. Among other factors, the authors give examples of fibromuscular dysplasia, systemic vasculitis, connective tissue diseases, infections, as well as trauma and post-traumatic changes, while the frequency of mycotic lesions does not exceed 4%.
The triggering factor in the formation of false aneurysms is currently considered to be damage in the form of a rupture of the inner and middle layers of the vessel walls (intima and media) with delimitation of blood by the adventitia or surrounding perivascular tissues (for example, as a result of pancreatitis, autoimmune or mechanical damage to the wall during endovascular, laparoscopic or surgical intervention). An example is intimal trauma with dissection of the vascular wall, as a rare complication during the surgical installation of an intra-arterial port for regional chemotherapy in the palliative treatment of unresectable cancer or metastatic liver disease.
Most publications provide data that among all cases of visceral aneurysms, the incidence of splenic artery aneurysm is 60%, followed by hepatic artery aneurysms (20%). However, in a comprehensive retrospective review of the literature and clinical observations from 1985 to 1995 conducted in 2002 at the Mayo Clinic, among all visceral branch aneurysms, the authors described 103 cases of hepatic artery aneurysms and 83 cases of splenic artery aneurysms. The authors associate these changes in the ratio, firstly, with the trend towards a wider use of percutaneous diagnostic and therapeutic manipulations, and secondly, with the wider use of computed tomography for blunt abdominal trauma, which has resulted in an increase in the number of accidental findings of “hidden” aneurysms, not manifesting themselves clinically.
Based on their morphology, hepatic artery aneurysms can be classified as fusiform or saccular. By location, the right hepatic artery is most often affected (47%), followed by the common hepatic artery (22%), the hepatic artery proper (16%), the left hepatic artery (13%) and the cystic artery (1%).
Diagnostics.
Hepatic artery aneurysms are in most cases diagnosed incidentally as a result of examining a patient for nonspecific abdominal pain or any concomitant disease. In some observations, survey photographs reveal a ring of calcification in the area of the right hypochondrium. With barium fluoroscopy, the disease can be suspected by deformation of the duodenum due to compression outside the organ by a space-occupying formation. When performing esophagogastroduodenoscopy (EGD), an aneurysm can simulate a submucosal formation of the duodenum protruding into the lumen; with the formation of an aneurysm-duodenal fistula, erosion or an ulcer can be determined at the apex of the formation.
The ultrasound picture is variable; it depends on the size of the aneurysmal sac and the degree of thrombosis. A true aneurysm is often a hypoechoic, round, single-chamber formation adjacent to the hepatic artery; the presence of several chambers in the formation indicates a false aneurysm. Color Doppler mapping in the presence of a “yin-yang” sign (due to the high-speed movement of blood “back and forth”) in the cervical region allows one to differentiate false aneurysms from true ones, however, this pattern can also occur with a true saccular aneurysm, in this case analysis images in a clinical context (history) allows us to differentiate false aneurysms from true saccular aneurysms. Ultrasound is a valuable diagnostic tool for identifying aneurysms due to its easy accessibility, non-invasiveness, low cost, speed of obtaining results, as well as the absence of ionizing radiation and the need for the use of contrast agents. The method has a sensitivity of 94% and specificity of 97% in detecting aneurysms. However, this method is operator dependent, and obtaining data from critically ill patients may be difficult.
Multidetector computed tomography is a valuable tool that allows you to clarify the topographic-anatomical relationship of the aneurysm with surrounding structures, study the anatomy of the vessels, obtain information about the condition of the vascular wall, assess the condition of the surrounding tissues and plan the tactics and scope of the upcoming intervention. True aneurysms on computed tomography scans of aneurysms, as a rule, have a fusiform shape, often extending over a significant length, involving the entire circumference and all three layers of the vessel wall. False aneurysms are usually saccular in shape with a narrow neck and have smooth, well-demarcated walls represented by blood delimitation by the adventitia or surrounding perivascular tissue. The presence of irregular walls with unclear boundaries and a wide neck suggests the mycotic nature of the aneurysm. On unenhanced examination, an aneurysm may appear as an isodense, rounded structure adjacent to the vessel. The introduction of a contrast agent indicates filling of the lumen of the aneurysmal sac, and the absence of complete filling may indicate the presence of parietal thrombotic masses. Computed tomography, unlike ultrasound, is an operator-independent method and has a shorter time for obtaining diagnostic images. However, post-processing the raw data and creating 3D reconstructions can be labor-intensive and require specialized software on the clinician's workstation. Computed tomography provides an assessment of the entire vascular bed, while subtraction angiography is limited to a selected vascular area, but, unlike it, has less spatial resolution. In a study by J. A. Soto et al., the sensitivity and specificity of the method were 95.1% and 98.7%.
Complications.
The most severe complication of this disease is the rupture of an aneurysm with the development of gastrointestinal bleeding and hemorrhagic shock, leading to death. Blood breakthrough can occur into the abdominal cavity (43%), into the lumen of the stomach and duodenum (11%), into the bile ducts (41%) or into the portal vein (5%). The risk of rupture with an aneurysm diameter greater than 2 cm reaches 50%, and the overall mortality due to rupture approaches 70%. An increase in the diameter of the aneurysm when choosing non-surgical management tactics was noted in 27% of cases and amounted to up to 0.8 cm over three years. In addition, it was noted that the risk of rupture of aneurysms resulting from non-atherosclerotic changes is much higher. Due to the high rate of spontaneous rupture, surgical treatment is indicated for aneurysms larger than 2 cm in diameter.
Treatment.
The first choice method in the treatment of hepatic artery aneurysms is endovascular intervention. The choice of treatment strategy depends on the location of the aneurysm. Aneurysms of the branches of the hepatic artery, as a rule, are filled with detachable coils or special adhesives (for example Onyx) without the risk of parenchymal ischemia, due to the double blood supply to the liver. Aneurysms of the common hepatic artery can be excluded from the blood flow by coils distal and proximal to the neck of the aneurysm, while the gastroduodenal artery will provide its own hepatic artery with sufficient blood flow. Aneurysms of the native hepatic artery and its bifurcation should be excluded from the bloodstream while maintaining vessel patency. With a wide neck of the aneurysm, it is possible to use balloon-assisted technology, when the detachable coils are held in its cavity using an inflated balloon catheter. There are several reports in the literature of successful implantation of flow redirection stents to exclude an aneurysm from the circulation. After the endovascular procedure, a follow-up study is recommended one month and six months later.
In the domestic literature, descriptions of cases of hepatic artery aneurysms are rare. Considering the rarity of this pathology, as well as the fact that the clinical picture does not have pronounced specificity and diagnosis before the development of life-threatening complications is difficult, we present our own clinical observation.
A 44-year-old patient was transported via emergency medical services to the emergency department of City Clinical Hospital No. 71 of the Moscow City Clinical Hospital with complaints of severe weakness, dizziness and repeated loss of consciousness for two weeks. Over the last 4 days, he has noticed the appearance of black stools. The day before, he had pain in the heart area that was not self-limiting, and therefore sought medical help.
Upon admission, the condition was stable and serious. The patient is conscious, communicative, and adequate. The skin is pale. Hemodynamics are stable. From laboratory data, normochromic anemia is noteworthy. When performing endoscopy, a moderate amount of “coffee grounds” and food is placed in the gastric lumen. The pylorus is passed, the duodenal bulb is deformed - along the upper wall there is compression from outside to 2/3 of the lumen without signs of independent or transmitted pulsation, at the top of which an ulcerative defect measuring up to 0.5 cm with fibrin at the bottom is determined.
Ultrasound of the abdominal cavity in the projection of the pylorus and duodenal bulb reveals a volumetric formation of a heterogeneous echostructure, measuring 56x36x57 mm. With CDK, the formation is avascular, the transmission pulsation is determined, distal to the formation is the common hepatic artery.
Computed tomography of the abdominal cavity with bolus contrast enhancement using a standard 3-phase protocol revealed expansion and tortuosity of the branches of the celiac trunk: common hepatic artery (to the level of the porta hepatis) up to 15 mm, thickening of the walls up to 5 mm, splenic artery up to 11 mm with thickening walls up to 13 mm. In the area of the duodenal bulb, a rounded formation up to 35 mm is determined, pushing aside the intestine, not separable along the dorsal contour from the hepatic artery. In the delayed phase, there is a slight accumulation of contrast in the capsule of the formation. In the lumen of the stomach and small intestine, against the background of contrasting contents, multiple clots are determined.
Conclusion: “rupture of a fusiform aneurysm of the common hepatic artery with a breakthrough of blood into the stomach or duodenum.”
By agreement, the patient was transferred to a specialized institution, where, as a result of relapse of profuse gastrointestinal bleeding, surgery was performed for emergency indications.
Intraoperatively, an aneurysmal dilatation of the hepatic artery up to 5-6 cm over a length of up to 5 cm was detected, ending at the bifurcation site. During the audit, it was found that there was a defect in the aneurysm wall along the lower edge, extending to the posterior wall of the stomach in the area of the pylorus and the initial parts of the duodenum with the formation of a “daughter” false aneurysm up to 4 cm, made with old and fresh bundles. A true aneurysm of the common hepatic artery was resected. The common hepatic artery was replaced with a 10 mm GORE-TEX prosthesis. The cavity of the false aneurysm is plugged with a strand of the greater omentum. The postoperative period was without complications. The patient was discharged on the 17th day in satisfactory condition.
Conclusion.
Aneurysms of the hepatic arteries are a rare pathology, and given the paucity and blurred clinical picture, to identify and verify this pathology it is necessary to use the entire available range of radiation imaging methods. The sequence of application of research methods should correspond to the increase in their invasiveness. Ultrasound examination at an early stage allows, without radiation exposure to the patient, to diagnose an aneurysm and evaluate the vessel that is its source. The diagnostic accuracy of computed tomography is comparable to the information content of traditional angiography and allows not only to clarify the relationship of the aneurysm with the surrounding structures, but also to assess the condition of the surrounding tissues, as a result of which it is reasonable to use it as the next stage of the diagnostic process not only to clarify the diagnosis but also to plan the scope of surgical treatment.
X-ray endovascular treatment is an effective method for achieving reliable exclusion of the aneurysm from the bloodstream; the type of intervention depends on the topographic and anatomical features of the aneurysm.
Late diagnosis of this pathology can lead to serious complications, including death.
The interest of the presented clinical observation is due, in our opinion, to the rare occurrence of the pathology and the convincingness of the data obtained using ultrasound and computed tomography.
Literature
- Huang Y. K., Hsieh H. C., Tsai F. C., Chang S. H., Lu M. S. Visceral artery aneurysm: risk factor analysis and therapeutic opinion. Eur J Vasc Endovasc Surg. 2007; 33: 293-301.
- Lesnyak V.N., Kemezh Yu.V., Ermicheva A.Yu. CT diagnosis of aneurysms of the visceral branches of the abdominal aorta. Russian electronic journal of radiology diagnostics 1: 65-70.
- Guida P. M., Moore S. W. Aneurysm of the hepatic artery. Report of five cases with a brief review of the previously reported cases. Surgery 1966; 60: 299-310.
- Crisp E. A Treatise on the Structure, Diseases and Injuries of the Blood-Vessels With statistical deductions, etc. John Churchil 1847;
- Friedenwald J., Tannenbaum K. Aneurysm of hepatic artery. American Journal of the Medical Sciences 1923; 11-28.
- Oser L., von Neusser E., Quincke H. I., Hoppe-Seyler G. K. F. Diseases of the Liver, Pancreas and Suprarenal Capsules:. Sanders 1905;
- Hale-White W. Common Affections of the Liver. Nisbet 1908;
- Messina L. M., Shanley C. J. Visceral Artery Aneurysms. Surgical Clinics of North America 1997; 77: 425-442.
- Shcherbyuk A., Artyukhina E., Ulyanov D., Frolov K., Zaitsev A., Zhao A. Hepatic artery aneurysm as a cause of obstructive jaundice. Doctor 2007; 12: 65-67.
- Kehr H. Der erste Fall von erfolgreicher Unterbindung der Arteria hepatica propria wegen Aneurysma. Munchen Med Wschr 1903; 1: 1861-1863.
- Gordon-Taylor G. Rare Cause of Severe Gastro-intestinal Haemorrhage. British medical journal 1943; 1:504.
- Siew S. Aneurysm of the hepatic artery; report of a case and review of the literature. S Afr J Clin Sci 1952; 3: 143-153.
- Barnett W. O., Wagner J. A. Aneurysm of the hepatic artery cause of obscure abdominal hemorrhage. Annals of surgery 1953; 137:561.
- Curran F. T., Taylor S. A. Hepatic artery aneurysm. Postgrad Med J 1986; 62: 957-959.
- Ikeda O., Tamura Y., Nakasone Y., Iryou Y., Yamashita Y. Nonoperative management of unruptured visceral artery aneurysms: treatment by transcatheter coil embolization. J Vasc Surg 2008; 47: 1212-1219.
- Kvashnin A. I., Atamanov S. A., Melnik A. V., Bykov O. A., Pomkin A. A., Shirkin M. G. Endovascular reduction of false aneurysm of the native hepatic artery. Clinical case. International Journal of Interventional Cardioangiology.
- Abbas M. A., Fowl R. J., Stone W. M., Panneton J. M., Oldenburg W. A., Bower T. C. et al. Hepatic artery aneurysm: factors that predict complications. J Vasc Surg 2003; 38: 41-45.
- Shanley C. J., Shah N. L., Messina L. M. Common splanchnic artery aneurysms: splenic, hepatic, and celiac. Ann Vasc Surg 1996; 10: 315-322.
- Sachdev-Ost U. Visceral artery aneurysms: review of current management options. Mt Sinai J Med 2010; 77: 296-303.
- O"Driscoll D., Olliff S. P., Olliff J. F. Hepatic artery aneurysm. Br J Radiol 1999; 72: 1018-1025.
- Man C. B., Behranwala K. A., Lennox M. S. Ruptured hepatic artery aneurysm presenting as abdominal pain: a case report. Cases J 2009; 2: 8529.
- Huang C-T, Chiu C-Y, Chen K-H, Lee T-H. A Common Hepatic Artery Aneurysm Mimicking A Duodenal Submucosal Tumor Presenting as Upper Gastrointestinal Bleeding: A Case Report. J Int Med Taiwan 2010; 21: 56-61.
- Shaw J. F. Hepatic artery aneurysms. Br J Hosp Med 1982; 28: 407-409.
- Chung-Tsui. C. H. A Common Hepatic Artery Aneurysm Mimicking A Duodenal Submucosal Tumor Presenting as Upper Gastrointestinal Bleeding: A Case Report. 2010; 51-56.
- Athey P. A., Sax S. L., Lamki N, Cadavid G. Sonography in the diagnosis of hepatic artery aneurysms. AJR Am J Roentgenol. 1986; 147: 725-727.
- Saad N. E., Saad W. E., Davies M. G., Waldman D. L., Fultz P. J., Rubens D. J. Pseudoaneurysms and the role of minimally invasive techniques in their management. Radiographics 2005; S173-189.
- Katyal S., Oliver J. H., 3rd, Buck D. G., Federle M. P. Detection of vascular complications after liver transplantation: early experience in multislice CT angiography with volume rendering. AJR Am J Roentgenol. 2000; 175: 1735-1739.
- Molina J. A., Benito Santamaría V., Guerrero R., Babun Y. Spectrum of CT Angiography Findings of Pseudoaneurysm. ECR 2013;
- Soto J. A., Munera F., Morales C., Lopera J. E., Holguin D., Guarin O. et al. Focal arterial injuries of the proximal extremities: helical CT arteriography as the initial method of diagnosis. Radiology 2001; 218: 188-194.
- Zatevakhin I.I., Tsitsiashvili M.Sh., Zolkin V.N., Sideltseva A.A. Rupture of hepatic artery aneurysm with the formation of a duodenal fistula.
- Carr S. C., Mahvi D. M., Hoch J. R., Archer C. W., Turnipseed W. D. Visceral artery aneurysm rupture. J Vasc Surg 2001; 33: 806-811.
- Wojtaszek M. Managing Visceral Artery Aneurysms. Endovascular today. 2013; 10: 77-81.
- Tarazov P. G., Ryzhikov V. K., Polysalov V. N., Prozorovsky K. V., Polikarpov A. A. Unsuccessful embolization of aneurysm of the common hepatic artery. Surgery 1998; 8:54-55.
- Timerbulatov V. M., Timerbulatov M. V., Ishmetov V. Sh., Chudnovets L. G., Mustafakulov U. S. Aneurysms of the visceral arteries of the abdominal cavity. Clinical and experimental surgery.
- Shcherbyuk A., Artyukhina E., Ulyanov D., Frolov K., Zaitsev A., Zhao A. Hepatic artery aneurysm as a cause of obstructive jaundice.
The hepatic artery is a branch of the celiac trunk. It passes along the upper edge of the pancreas to the initial part of the duodenum, then goes up between the leaves of the lesser omentum, located in front of the portal vein and medial to the common bile duct, and at the porta hepatis it divides into right and left branches. Its branches also include the right gastric and gastroduodenal arteries. Additional branches are often found. Topographic anatomy has been carefully studied on donor livers. With abdominal trauma or catheterization of the hepatic artery, its dissection is possible. Embolization of the hepatic artery sometimes leads to the development of gangrenous cholecystitis.
Clinical manifestations
The diagnosis is rarely made while the patient is alive; There are few works describing the clinical picture. Clinical manifestations are associated with an underlying disease, for example, bacterial endocarditis, periarteritis nodosa, or are determined by the severity of upper abdominal surgery. Pain in the epigastric region on the right occurs suddenly and is accompanied by shock and hypotension. There is pain on palpation of the right upper quadrant of the abdomen and the edge of the liver. Jaundice increases rapidly. Typically, leukocytosis, fever, and biochemical blood tests reveal signs of cytolytic syndrome. Prothrombin time increases sharply, bleeding appears. When large branches of the artery are occluded, a coma develops and the patient dies within 10 days.
It is necessary to carry out hepatic arteriography. It can be used to detect hepatic artery obstruction. Intrahepatic collaterals develop in the portal and subcapsular areas. Extrahepatic collaterals with neighboring organs are formed in the ligamentous apparatus of the liver [3].
Scanning.Infarctions are usually round or oval, occasionally wedge-shaped, located in the center of the organ. In the early period, they are detected as hypoechoic foci during ultrasound examination (ultrasound) or poorly demarcated areas of reduced density on computed tomograms that do not change with the introduction of a contrast agent. Later, heart attacks look like confluent foci with clear boundaries. Magnetic resonance imaging (MRI) allows you to identify infarcts as areas with low signal intensity on T1-weighted images and with high intensity on T2-weighted images. With large infarcts, the formation of “lake” of bile, sometimes containing gas, is possible.
Treatment should be aimed at eliminating the cause of the damage. To prevent secondary infection during liver hypoxia, antibiotics are used. The main goal is the treatment of acute hepatocellular failure. In case of arterial injury, percutaneous embolization is used.
Damage to the hepatic artery during liver transplantation
When the bile ducts are damaged due to ischemia, they speak of ischemic cholangitis.It develops in patients who have undergone liver transplantation due to thrombosis or stenosis of the hepatic artery or occlusion of the paraductal arteries |8[. Diagnosis is complicated by the fact that the picture when examining biopsy specimens may indicate obstruction of the bile ducts without signs of ischemia.
After liver transplantation, hepatic artery thrombosis is detected using arteriography. Doppler examination does not always reveal changes; moreover, correct assessment of its results is difficult [b]. The high reliability of spiral CT has been shown.
Hepatic artery aneurysms
Hepatic artery aneurysms are rare and account for one fifth of all visceral vessel aneurysms. They may be a complication of bacterial endocarditis, periarteritis nodosa, or arteriosclerosis. Among the causes, the role of mechanical damage is increasing, for example due to road traffic accidents or medical interventions such as biliary tract surgery, liver biopsy and invasive X-ray examinations. False aneurysms occur in patients with chronic pancreatitis and pseudocyst formation. Hemobilia is often associated with false aneurysms. Aneurysms are congenital, intra- and extrahepatic, ranging in size from the head of a pin to a grapefruit. Aneurysms are identified by angiography or discovered incidentally during surgery or autopsy.
Clinical manifestations varied. Only a third of patients have the classic triad: jaundice |24|, abdominal pain and hemobilia. A common symptom is abdominal pain; the period from their appearance to the rupture of the aneurysm can reach 5 months.
In 60-80% of patients, the reason for the initial visit to the doctor is the rupture of a modified vessel with the leakage of blood into the abdominal cavity, biliary tract or gastrointestinal tract and the development of hemoperitoneum, hemobilia or hematemesis.
Ultrasound allows you to make a preliminary diagnosis; it is confirmed using hepatic arteriography and contrast-enhanced CT (see Fig. 11-2). Pulsed Doppler ultrasound can detect turbulence of blood flow in the aneurysm.
Treatment. For intrahepatic aneurysms, vessel embolization is used under angiography control (see Fig. 11-3 and 11-4). In patients with aneurysms of the common hepatic artery, surgical intervention is necessary. In this case, the artery is ligated above and below the site of the aneurysm.
Hepatic arteriovenous fistulas
Common causes of arteriovenous fistulas are blunt trauma to the abdomen, liver biopsy or tumors, usually primary liver cancer. Patients with hereditary hemorrhagic telangiectasia (Randu-Weber-Osler disease) have multiple fistulas, which can lead to congestive heart failure.
If the fistula is large, a murmur can be heard over the right upper quadrant of the abdomen. Hepatic arteriography can confirm the diagnosis. Embolization with gelatin foam is usually used as a therapeutic measure.
Length of proper hepatic artery ranges from 0.5 to 3 cm, diameter from 0.3 to 0.6 cm. With a small diameter of the native hepatic artery, accessory hepatic arteries are usually observed. The right gastric artery departs from its own hepatic artery; less often, it gives branches to the gallbladder, duodenum and pylorus. In the middle third of the hepatoduodenal ligament, the proper hepatic artery is divided into two, sometimes three hepatic branches.
The right hepatic branch has a length of 2-4 cm, a diameter of 0.2-0.4 cm, more often it is located posterior to the common hepatic duct, less often - anterior to it. In most cases, it gives off the gallbladder artery, a. cystica, and, heading towards the right lobe of the liver, is located near the neck of the gallbladder. Sometimes there are two branches going to the right lobe of the liver. In such cases, one of them may be located anteriorly and the other posteriorly to the common hepatic duct.
Options are also observed when the right branch of the hepatic artery is located below the common hepatic duct and crosses the common bile duct on its way.
Left hepatic branch is directed to the left part of the transverse groove, supplying blood to the left, often quadrate, as well as the caudate lobes of the liver. Its length is approximately the same as the right branch (2-3 cm), and its diameter is slightly smaller - 0.2-0.3 cm.
Right and left hepatic branches near the gate or in the liver parenchyma they are divided into second-order branches, which in the substance of the liver are in turn divided into smaller branches.
“Atlas of operations on the abdominal wall and abdominal organs” V.N. Voylenko, A.I. Medelyan, V.M. Omelchenko
Often the greater omentum is adjacent to the liver or fused with it. Such adhesions are often observed in the area where the gallbladder is located. Between the diaphragm and the upper surface of the right lobe of the liver there is a slit-like space - the hepatic bursa, which from above reaches the coronary ligament of the liver and is separated from the pregastric bursa by the falciform ligament. At the bottom, the bag communicates with the preomental space, and with...
The extrahepatic bile ducts include: right and left hepatic, common hepatic, cystic and common bile. At the gate of the liver, the right and left hepatic ducts, ductus hepaticus dexter et sinister, emerge from its parenchyma. The left hepatic duct in the liver parenchyma is formed by the fusion of the anterior and posterior branches. The anterior branches collect bile from the quadrate lobe and from the anterior...
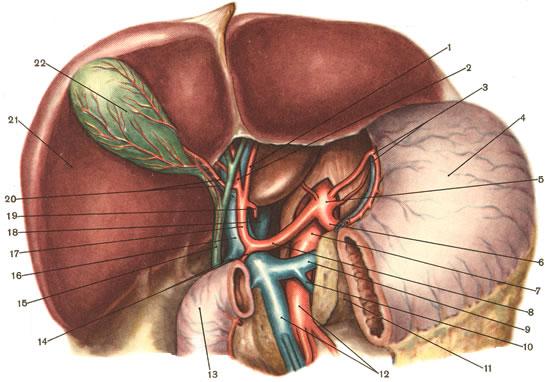
Blood supply. Blood flows to the liver from two sources: the hepatic artery and the portal vein. Blood vessels of the liver and gall bladder (stomach and pancreas are partially excised) I - ramus sinister a. hepaticae propriae; 2 - ramus dexter a. hepaticae propriae; 3 - a. et v. gastrica sinistra; 4 - ventriculus; 5 - truncus coeliacus; 6 - a….




