Hernia of the white line of the abdomen in children is treated without surgery. Linea alba in a child and the reasons for the formation of a hernia on the abdomen. Symptoms of a hernia in a child
During embryogenesis, at various stages of fetal development, some elements, layers of tissue of the white line of the abdomen, are not formed correctly and completely. These defects include aplasia of the anterior abdominal wall, hernias of various locations (inguinal, umbilical, embryonic, diaphragmatic). Hernia of the white line of the abdomen occurs mainly in adult children (more often in children 5-7 years old). It is rarely infringed and does not tend to close on its own.
Causes
There are many factors that contribute to the occurrence and even progression of this pathological condition. A hereditary tendency leads to the occurrence of hernias; in fact, it is the most common cause of all ailments. The linea alba, which runs from the xiphoid process to the pubis, is the line of intersection of the aponeuroses of the rectus abdominis muscles. This is where hernias can form.
There are factors that increase intra-abdominal pressure and circumstances that weaken the anterior abdominal wall. The latter include weight loss, abdominal trauma, abdominal surgery and diseases that deplete children.
Factors that increase abdominal pressure:
- Postoperative scars on the tummy;
- Hereditary tendency;
- Obesity;
- Constant constipation;
- Prolonged hacking cough or screaming;
- Physical overexertion;
- Ascites.
Long-term exposure to causes on the child’s small body leads to weakening of the aponeurosis and muscles of the abdominal wall.
Mechanism of hernia formation
The occurrence of a hernia is associated with the unfinished development of the aponeurosis, in which gap-like defects remain. These defects exist for the passage of nerves and blood vessels through them, connecting the preperitoneal fatty tissue with the subcutaneous tissue. A typical and characteristic place for the occurrence of a pathological condition called a hernia is considered to be the upper region of the white line; peri-umbilical (paraumbilical) and hypogastric localizations are very rarely found.
During an increase in intra-abdominal pressure, pre-abdominal fatty tissue falls out, which is later called preperitoneal lipoma. When this lipoma is compressed, acute pain occurs.
This pain syndrome can be confused with similar symptoms in conditions such as inflammation of the pancreas, gall bladder, peptic ulcer, peritonitis or other abdominal pathologies. Later, the peritoneum falls out and a hernial sac is formed, into which the internal organs emerge. This moment is the formation of a true hernia. Accordingly, there are three stages of development of a hernia of the white line of the abdomen:
- preperitoneal lipoma;
- initial stage;
- formed hernia.
O.P. Krymov identifies types of hernia of the white line of the abdomen, depending on its location:
- supra-umbilical (hernia epigastrica);
- subumbilical (hernia paraumbilicalis);
- peri-umbilical (hernia hypogastrica).
The latter type is very rare, because this is facilitated by the anatomical features of the white line itself, which narrows and thickens below the navel, so defects are less likely to form here. Very rarely, a child may develop not one, but several hernias of the white line of the abdomen. In this case, the pathology is called multiple hernias.
If the hernia is large, most often its contents will be the omentum, loops of the small intestine, and sometimes the wall of the transverse colon.
Symptoms
Most often, the hernia is asymptomatic, and is found by parents or doctors during a routine examination.
A rounded protrusion will be noticeable along the midline, smooth and elastic to the touch, which increases during sneezing, coughing, or lifting weights; if you press on it, it can decrease. The protrusion may also decrease when lying down. As for the pain, it is mainly localized in the upper abdomen and intensifies with pressure, straining and after eating. Parents should also be wary of digestive disorders. This includes complaints of nausea, vomiting, heartburn, and constipation.
Research methods
- examination and history taking of a small patient;
- auscultation (listening), palpation (feeling) of the hernia;
- general blood and urine analysis;
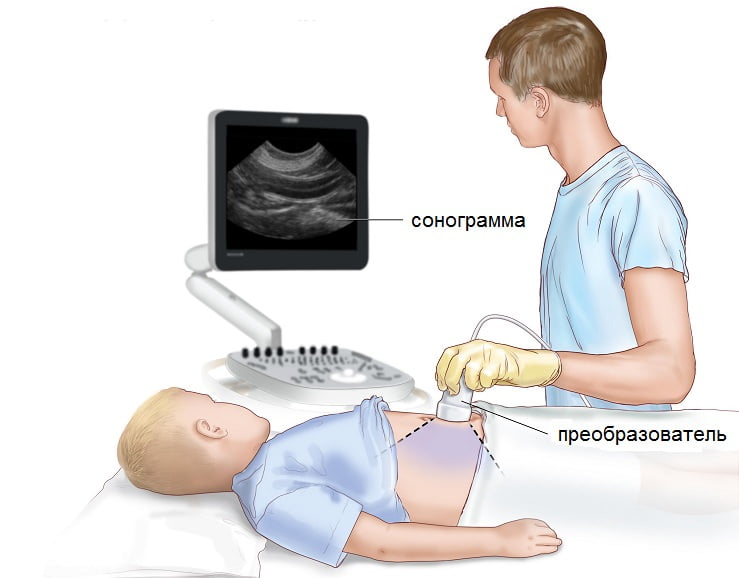
- Ultrasound of the contents of the hernial sac;
- gastroscopy;
- X-ray examination of the abdominal organs;
- herniography;
- CT or MRI in difficult situations.
Ultrasound of the white line of the abdomen is considered a very safe and informative research method. It is used to clarify the nature and location of the hernia defect, and to clarify the contents of the hernial sac.
Abdominal palpation procedure to identify a hernia of the linea alba
Differential diagnosis should be carried out with the following diseases:
- Peptic ulcer of the stomach/duodenum;
- Gastritis;
- Appendicitis;
- Cholecystitis;
- Pancreatitis;
- Tumor metastasis to the omentum.
This requires detailed instrumental and laboratory diagnostics of the digestive system.
Possible complications
- Strangulated hernia. The problem with this is poor circulation in the organs that are located in the hernial sac. The consequence will be intestinal gangrene. Moreover, the inflammatory process begins to intensify, quickly spreading to neighboring organs. And this will already indicate diffuse peritonitis.
- Irreversible hernia. It is characterized by the fact that it is not possible to reduce the hernial contents. This is explained by the fusion of the organs of the hernial sac with each other.
- Injury to the formation is dangerous due to subsequent damage and inflammation of the abdominal organs.
How to cure?
Any mother should immediately consult a surgeon. He will do everything necessary for further diagnosis and treatment of your child.
Doctor's note: Even with small hernias, you must be observed by a surgeon, because there is a high risk of strangulation of the hernia.
Treatment of hernia of the white line of the abdomen only by surgery. This operation is called hernioplasty. It is planned and not very complicated. All surgical procedures are performed only under general anesthesia. Now surgeons use modern and child-safe means to ensure that young patients tolerate operations well.
Doctor's note: Traditional methods of treating hernias in children concern only umbilical hernias in the early stages of the disease. An abdominal bandage does not treat a hernia if it has already appeared.
Surgery as a method of treating hernia of the white line of the abdomen
Depending on the stage of the disease, local or artificial material is used. The surgeon must correct diastasis (separation of the rectus abdominis muscles). If local fabrics are used, the defect is eliminated using a synthetic thread. This method often leads to the reappearance of the hernia because the load on the sutures is quite large. Therefore, during surgery, synthetic mesh frames or prostheses are often used, which cover the aponeurosis and the load on the sutures becomes uniform. The likelihood of relapse when using these frames is almost zero.
The procedure lasts on average 25-40 minutes, it depends on the complexity and scope of the surgical procedure.
A few hours after the operation, children and their parents have the opportunity to return home. The stitches are removed after a week or a week and a half.
Postoperative period
After the surgical procedure, you must follow a restrictive regime for three days, and limit physical activity for 20 days.
Diet you need to follow:
- You can’t eat fatty, fried, spicy foods;
- liquid foods such as cereals, soups, vegetable or chicken broths, purees, and fermented milk products facilitate the baby’s digestion process;
- to restore strength and improve peristalsis, you need to add juices, fruit and vegetable purees to your diet;
- Flatulence and colic can occur with excessive fiber intake.
Prevention
Prevention in infants is to prevent constipation. The child should not overeat and scream. Adult children are recommended to play sports, this helps to tighten the aponeurosis.
To prevent relapses and reduce pressure on the abdominal wall, you can use a bandage.
In the case of a hernia of the linea alba, timely diagnosis and treatment is considered very important and necessary, otherwise complications are inevitable. Surgical intervention will allow you to completely get rid of the disease.
Have you noticed a strange protrusion in the center of your child’s abdomen? It could be a hernia of the linea alba.
During the formation of the fetal abdominal wall (surrounding the organs), the abdominal muscles formed an aponeurosis - a tendon plate, which is the attachment point of the two rectus muscles. In fact, it is a muscle tendon, only devoid of nerve endings and blood vessels. It runs vertically from the xiphoid process to the inguinal fold strictly in the middle. During embryonic development, some processes are disrupted and the aponeurosis becomes less strong; thinning defects remain at birth. It is in these thin places that hernias of the white line of the abdomen form.
Causes
Typically, such hernias begin to appear with age, because the hernia forms over time with constant stress on the abdominal muscles. This may include frequent constipation, prolonged hacking cough (for example, with chronic bronchitis or severe whooping cough) and the cry of a child. Obesity, ascites (swelling), trauma and physical stress in this area also negatively affect the aponeurosis. There is a risk of developing a hernia after surgery on the anterior abdominal wall. It is worth noting that hernia occurs more often in boys.
Stages
The hernia also does not suddenly break through the aponeurosis; it is formed over a certain period of time, going through three stages of evolution:
- Stage of lipoma in the tissue. There is no hernial sac yet; a small accumulation of adipose tissue grows preperitoneally above the aponeurosis.
- The stage of the beginning of pouch formation. The walls of the thinned defect diverge, and a hernial protrusion begins to form from the peritoneum.
- The stage of a fully formed hernia. The leaves of the peritoneum fall into the defect, forming a pocket - a hernial sac. Nearby organs can get into it under pressure. The most common content, due to its adherence to the anterior wall, is the greater omentum; somewhat less frequently, one or more loops of the small intestine and other organs are included.
The linea alba is about twenty to thirty centimeters long. The wall defect can be anywhere along this line and of any size. It is customary to divide the localization into three zones: above the navel, below it and the peri-umbilical region.
The strongest part of the aponeurosis is located under the navel, so hernias in this area are rare. Above and around the navel (paraumbilical) is the most possible place for a hernia to form. Sometimes difficulties arise in distinguishing between umbilical hernias and hernias near the navel, since their protrusions look the same, but with proper palpation it becomes clear that the cause is a defect in the wall. In the presence of several defects, multiple hernias may occur along the length from the lower process of the sternum to the navel. All this depends on the presence of initial pathology and trigger factors during life.
Clinical picture
Hernias of the white line of the abdomen are diagnosed very often in children older than 2-3 years. Sizes vary from small, no more than a centimeter, to giant hernias. In the midline of the abdomen, a round, smooth elastic formation is visible to the naked eye, most often painless and easily reducible. Typically, only preperitoneal fatty tissue extends into the aponeurosis defect. Also, the expansion of connective tissue causes diastasis (separation) of the rectus muscles on the abdomen. In case of complications, painful sensations may occur that are associated with the entry of a layer of parietal peritoneum into the hole in the aponeurosis, forming a hernial sac. It has its own nerve endings that can react and cause pain.) If the hernial sac has contracted and the contents have not had time to go back into the intra-abdominal cavity, then a strangulation of the hernia of the white line of the abdomen occurs, which is accompanied by an inflammatory reaction, severe pain and impaired intestinal motility. Although it is worth noting that in children such a complication is an extremely rare occurrence due to the elasticity of the abdominal walls.
If a child develops symptoms such as weakness, sudden single vomiting, severe nausea, severe pain in the center of the abdomen, the hernia does not self-reduce in a horizontal position, and there are streaks of blood in the stool - immediately go to a surgical hospital!
Diagnostics
Diagnosing a white line hernia is not particularly difficult. A characteristic clinical picture, collecting complaints from the child or his parents and determining the location of the defect by palpation almost always makes it possible to make the correct diagnosis. To confirm, ultrasound is most often used, which confirms the presence of a defect and allows you to determine the type of contents in the hernial sac. If the doctor has any doubts, or there is a suspicion of a strangulated hernia, then the hospital can use diagnostic methods such as X-ray examination of the stomach, MRI or MSCT. They will help differentiate a hernia from intestinal obstruction or make an accurate diagnosis.
Treatment
Treatment of a hernia of the white line of the abdomen, including the peri-umbilical one, is only surgical. If a hernia is detected at an early age (1-2 years) or in a newborn, pediatric surgeons recommend refraining from immediate surgery because at this age the muscles of the anterior wall are still forming and self-healing is possible. Parents are recommended to massage the child’s tummy and buy him a special corset that will support and protect the aponeurosis from excessive pressure from the inside. At a later age, such measures are compensatory in nature; they no longer eliminate the disease, they only restrain its development.
The operation is performed after diagnosis. If you delay resection of the hernia, there may be a risk of complications or further increase in the protrusion. After passing clinical blood and urine tests and establishing the exact location of the injury, the child is admitted to a surgical hospital and is operated on in a day or two.
Photo of removal of hernia of the white line of the abdomen. Click on + to view

Contraindications to surgery are severe systemic diseases and the presence of an infectious agent in the body. Then the patient is discharged for further treatment and after complete recovery can lie down on the operating table.
Surgeries to remove a hernia are called hernioplasty. Both traditional open surgical interventions and modern endovideosurgical methods can be performed. All plastic surgeries are performed under general (intravenous or mask) anesthesia.
Open types of operations
1 Tension hernioplasty (own tissue is used). This is a classic method developed back in the last century. It is used for resection of small hernias without pronounced diastasis. After incision of the skin and pancreas, the aponeurosis defect is sutured with special non-absorbable threads made of catgut. They are also the weak point of this operation - under heavy loads the seam can come apart. If the hernia recurs, dangerous complications may occur, such as bleeding, strangulation and necrosis of the hernial sac. 2 Tension-free plastic surgery (use of special mesh implants). This method appeared after the invention of polymer materials that are inert enough to remain in the body for a lifetime without causing rejection. A mesh fabric made of this material is used to cover the hole in the connective tissue and sutured to the edges of the abdominal muscles. This operation provides high reliability and does not reduce the child’s quality of life. Another advantage is the low probability of relapse (less than one percent) and short rehabilitation. During surgery, it is also possible to close the discrepancy of the rectus abdominis muscles.Video
This video presents a variant of hernia repair using mesh.
Closed view of the operation
A high-tech and safe method of hernia resection is endoscopic hernioplasty. The intervention in the body is carried out not through a surgical incision, but through 3 small punctures of the skin. Carbon dioxide is injected into the abdominal cavity to create space between the internal organs and the anterior abdominal wall. Using special delicate manipulators, under video control, the mesh endoprosthesis is sutured to the abdominal wall from the inside. Depending on the doctor's skills, the operation is performed in a minimum amount of time. The undoubted advantages will be the absence of postoperative scars, painlessness and minimal rehabilitation time. The child can begin to engage in physical activity within 4-5 days. The risks of relapse are reduced to almost zero, since the patch installed from the inside can withstand greater pressure.
Video
This video is a recording from a video camera during endoscopic hernioplasty of the white line of the abdomen. By displaying the image on the screen, the surgeon navigates the abdominal space and performs the operation.
Prevention of hernia
To prevent the development of the process of hernia formation, the following recommendations will be useful to parents after the birth of their child.
Since stagnation of intestinal contents and excess weight increase the load on the anterior abdominal wall, make sure that the child has regular bowel movements and prevent constipation. For this purpose, pharmacies sell special gas tubes and drops for better digestion. Do not overfeed the baby, control his weight. Massage your abdominal muscles.
Try not to let your baby go for long periods of time without crying.
A hernia of the linea alba in children is diagnosed much less frequently than in adults. The linea alba is a strip of muscle fibers that originates from the xiphoid process of the chest, passes through the umbilical zone and ends at the symphysis pubis.
The occurrence of a hernia is caused by the divergence of the tendon plate bundles in the navel area, through which the intestinal loops protrude. The wider the divergence of the fibers, the less likely it is to get pinched.
Inguinal and umbilical hernias are much more common in newborns than in adults. According to statistics, hernia of the white line of the abdomen accounts for approximately 1% compared to similar diseases. The pathology can be congenital, developing during embryogenesis, or acquired.
Causes
Like any other disease, a hernia of the white line of the abdomen occurs as a result of objective reasons. Signs of the disease appear due to underdevelopment of the aponeurosis - the tendon plate of the abdominal wall. In this case, gaps appear in the tendon plate through which blood vessels and nervous tissue pass. Extrusion of preperitoneal tissue occurs due to increased pressure in the abdominal cavity.
Congenital
A congenital hernia occurs against the background of weakness of the anterior abdominal wall. This defect develops in utero during the formation of internal organs. Most often, the cause of the disease is a genetic predisposition.

Purchased
The development of a hernia in children can also occur at a later age. Among the factors that can trigger this process are:
- chronic constipation;
- excess weight;
- bronchitis;
- formation of postoperative scars;
- physical exercise;
- dropsy of the abdomen;
- severe coughing or screaming.
More often the disease is diagnosed in boys.
Symptoms of hernia of the white line of the abdomen
A clear sign of an abdominal hernia is pain in the epigastric region, accompanied by severe discomfort. The presence of pathology is indicated by a protrusion that disappears when the body is in an upright position.
Manifestations may vary depending on the severity of the disease and the location of the hernia.




However, there are the main symptoms by which one can judge what pathology is developing:
- constant aching pain;
- functional gastrointestinal disorders: attacks of nausea, vomiting, diarrhea;
- urinary disorders that can occur if the bladder gets into the hernial sac;
- increased body temperature, indicating the development of an inflammatory process;
- bloating.
If such symptoms occur, you should immediately consult a doctor.
Diagnostics
Diagnosis of the white line of the abdomen in children is carried out on the basis of examination and questioning of the patient. In addition, instrumental research methods can be used, such as:
- X-ray;
- Ultrasound of the hernial sac;
- gastroscopic examination;

To determine the pathology, specialists only need to complain from the child and indicate the painful area. With palpation, it is possible to make the correct diagnosis in almost every case.
Instrumental examination allows not only to confirm the diagnosis, but also to identify the location of the strangulated hernia.
Stages of the disease
Abdominal hernia in children goes through several stages of development. There are three stages of the disease:
- preperitoneal lipoma;
- initial stage;
- formed hernia.
It is advisable to consider the stages of development of protrusion in more detail.
Preperitoneal lipoma
The first phase of hernia development in children is characterized as preperitoneal lipoma. In medical practice, this pathology is called epigastric hernia. The formation is located in the hernial sac. It is small in size. Pain and discomfort in this case arise as a result of pinching of the hernia.
The main feature of preperitoneal lipoma is the tendency to fusion, which is an obstacle to its reduction.

Among the characteristic signs of this stage are:
- severe pain in the abdominal area, which in its manifestations is similar to colic;
- poor appetite;
- constant nausea;
- constipation
The disease at this stage is diagnosed by palpation, and treatment is carried out through surgery.
initial stage
In the absence of proper treatment, preperitoneal lipoma progresses to the initial stage, a characteristic feature of which is the presence of bulging of preperitoneal tissue through discrepancies in the tendons. At this stage, the hernia may stop developing and not progress, although sometimes the lipoma transforms into a hernial sac.
Formed hernia
A hernia at the stage of final formation is clearly visible and easily identified by palpation, despite the fact that it reaches large sizes only in some cases.

Hernias of the white line of the abdomen are classified depending on the level of location. Among them are:
- Supra-umbilical epigastric hernias located above the umbilical zone.
- Paraumbilical - formed near the navel. This is the rarest pathology.
- Infraumbilical hernias are located below the umbilical ring.
Hernias of the white line of the abdomen in most cases develop as isolated manifestations. Multiple pathologies are rare.
Surgical treatment
Any hernia can be eliminated only through surgery. Drug treatment and physiotherapeutic procedures cannot solve this problem.
Using conservative methods, you can only alleviate the child’s condition and slow down the progression of the disease.
The indication for surgery is the presence of a characteristic protrusion, on the basis of which the diagnosis was made. Surgical intervention to remove the protrusion is called hernioplasty.
Preparation
Before resorting to such methods, the doctor conducts an examination, assesses the possible risks and the degree of usefulness of the operation. Based on these data, a decision may be made not to perform the operation. This is possible if there is a minimal probability of a hernia being pinched and the general condition of the child’s body is normal.

The preparatory stage before the operation involves conducting studies, the list of which includes:
- taking general and clinical blood and urine tests;
- fluorography;
- electrocardiogram;
- Ultrasound of the abdominal cavity.
During the examination, it is mandatory to determine the patient’s blood type, blood clotting, the presence or absence of syphilis and hepatitis in the anamnesis, as well as determine whether the child is HIV-infected or not.
In some cases, additional examination is carried out.
Surgery can be performed under either local anesthesia or general anesthesia. The rehabilitation period takes no more than 1 week.
Rehabilitation
The postoperative rehabilitation period requires compliance with certain rules:
- minimizing physical activity;
- dieting.

These measures are necessary in order to bring the child’s body back to normal after hernioplasty. During the rehabilitation period, great importance is given to organizing proper nutrition. Spicy, fatty, fried foods, smoked foods, coffee, preservatives, pickles and chocolate are excluded from the diet.
Complications and consequences
In most cases, hernioplasty for a hernia passes without consequences, although some of them may appear. The most common complications include:
- development of inflammation, accompanied by a purulent course;
- recurrent process;
- collateral injury to nearby organs, nerve bundles or vascular walls;
- formation of adhesions;
- rejection of the implant used to close the gap or its displacement.
Hernioplasty to remove small hernias can be performed using your own tissue. This surgical procedure is called tension plasty. Hernioplasty using an endoprosthesis is the most effective treatment method and is carried out to remove small and medium-sized hernias. This type of surgery has several advantages.
Currently, the most common surgical problem in children is hernia. These are defects in the development of the abdominal walls, into which the abdominal organs (intestinal loops, bladder) or the intestinal fixing apparatus - the omentum - protrude. A hernia can be caused by many causes and factors that contribute to the onset and progression of this pathological condition. In order not to be afraid of this obscure illness and to be ready to get rid of it, it is recommended that you first prepare yourself informationally for the fight.
Reasons for development and structure
A hernia consists of a hernial sac, hernial contents and a hernial orifice, into which the sac with its contents prolapses. The most common cause of hernias is considered to be a hereditary predisposition.
information It is important to note that boys suffer from this disease much more often than girls.
Classification of hernias
Hernias are classified:
- By localization (that is, the place of its origin):
- diaphragmatic;
- intervertebral;
- femoral;
- hernia of the white line of the abdomen;
- ventral postoperative hernia.
- Size.
- The degree of its safety (meaning that sliding, reducible hernias are defects that require routine treatment, and strangulated hernias require immediate surgical correction).
Umbilical hernia
Most often it makes itself felt in the earliest period of a child’s development - neonatal or in the first months of life, when the umbilical remnant falls off and the wound heals. Most often it is formed due to the anatomical weakness of the umbilical ring, its incompetence. In addition to genetic predisposition, the causes of this type of hernia include:
- unsuccessful umbilical cord ligation;
- catheterization of the umbilical vein for health reasons;
- intestinal hyperpneumatosis (excessive gas formation);
- increased intra-abdominal pressure;
- diseases that reduce muscle tone (rickets, malnutrition, asthenia).
An umbilical hernia quite often protrudes when the child is restless, crying, straining, or constipated, but it is easily reducible and is very rarely strangulated. Clinically, it appears as a round or oval protrusion in the umbilical area with or without divergence of the rectus abdominis muscles. It can be of completely different sizes, and they can also increase or decrease. Many parents often perceive such an anatomical feature as a protruding navel as a hernia, but this is not true. But in any case, it is worth consulting with a pediatrician and pediatric surgeon regarding issues of concern.
information According to the experience of specialists from all over the world, we can say with confidence that in most cases this disease heals itself. In some children this occurs by the age of 1-2 years, in some it lasts until primary school age.
Hernia elimination is facilitated by:
- early placement of the baby on the tummy, when the abdominal wall is strengthened;
- physiotherapy;
- gymnastics;
- massage.
Surgical correction is indicated in cases of strangulation or large defect sizes. In a planned manner, operations are usually indicated from the age of five; operations are rarely accompanied by complications or relapses of the disease.
Inguinal hernia
This is also a common type of hernia and occurs much more often in boys; it practically never occurs in girls.
The causes may also be:
- heredity;
- features of the anatomy of the groin area;
- weakness of the abdominal muscles;
- non-fusion of the peritoneal process, which forms the inguinal canal.
It is a protrusion in the area of the inguinal canal; its hernial sac may also contain an omentum, loops of intestine, bladder wall, ovary (in girls) or spermatic cord (in boys). This type of hernia is strangulated more often than the previous one and requires emergency surgery.
dangerous An inguinal hernia in girls threatens necrosis (death) of the ovary, so it is extremely important to consult a surgeon if this occurs.
As planned, hernia repair begins when the child reaches 1 year of age or weighs at least 10 kg, when he is ready to adequately tolerate anesthesia. Modern surgery will provide the baby with a gentle operation, minimal blood loss and high-quality cosmetic stitches. Complications and relapses occur only if the doctor’s recommendations are not followed.
Hernia of the white line of the abdomen
The linea alba is an anatomical formation that is located vertically from the xiphoid process of the sternum to the pubic joint and is a connective tissue formation that connects the rectus abdominis muscles. In its structure there are several jumpers, if they diverge, a hernia is formed. Most often, they form just above the navel in fairly well-fed children with increased intra-abdominal pressure. The contents are a protective layer of adipose tissue in front of the outer layer of the peritoneum. Infringement of it threatens tissue necrosis. Treatment is only surgical, both planned and urgent.
Diaphragmatic hernia
This is the most dangerous type of hernia. It is rare, most often in combination with multiple malformations. The mortality rate for this type of hernia is high.
information A diaphragmatic hernia occurs when the membrane between the chest and abdominal cavities fails, as a result of which the abdominal organs are displaced into the chest and compress the lungs, causing them to collapse and increase pressure in the pulmonary artery, displacement and compression of the heart.
Usually the disease is diagnosed on the first day of a child’s life and is operated on urgently. The recovery period after successful completion of the operation is usually long, requiring long-term drug therapy, artificial ventilation, and parenteral nutrition (nutrient solutions in the form of intravenous infusions).
Symptoms
Symptoms of strangulation of any of the hernias (except diaphragmatic) are:
- Pain in the area of the protrusion, aggravated by pressure.
- Increased body temperature, feeling of chills, weakness.
- Change in skin color over the affected area from bright pink to purple-bluish.
- Inability to reduce the hernia back into the abdominal cavity.
- Feelings of tingling or bursting in the hernia.
important In this case, you should urgently seek help from a doctor. The sooner the child receives medical care, the less likely there are complications. Self-medication and traditional methods are a stupid waste of precious time.
Features of the postoperative period and consequences
After hernia repair and repair, relapses are possible if you do not adhere to the doctor’s strict recommendations, so the child needs to create the most comfortable conditions for recovery and rehabilitation. It is important to adhere to a diet, limit physical activity that can cause an increase in intra-abdominal pressure, engage in physical therapy with the baby during the recovery period, and undergo a course of restorative massage. Caring for the baby, patience, love and understanding will help solve the problem of hernia recurrence and make the little person’s childhood happy and joyful.
A hernia of the white line of the abdomen in children (epigastric hernia) is a protrusion of the hernial sac that appears through the aponeurosis in the anterior wall of the abdomen. Removing a hernia requires highly skilled surgery.
Mechanism of hernia formation

A hernia of the white line of the abdomen appears in the area of the so-called. The white line is a tendon strip that runs from the xiphoid process to the pubic fusion. The linea alba is wider in the upper part of the abdomen and narrows in the lower part, so the risk of a hernia is higher here.
When a hernia appears, the tendon fibers may diverge along the white line by 10-12 cm (diastasis). There is a possibility of diastasis turning into an umbilical hernia.
The shape of the hernial orifice can be round, oval or diamond-shaped. The narrower they are, the greater the likelihood of hernia strangulation. With reducible hernias, palpation of the hernial orifice is possible.
Unlike other types of hernias, a hernia of the linea alba in a child is quite rare (approximately 0.8% of cases). It usually occurs after 5 years of age due to insufficient development of the aponeurosis. As a result, gaps may appear in the tendon bridges. A strangulated hernia occurs rarely.
Often, a hernia of the white line is single, but in some cases several hernias are observed, which are located one above the other.
Symptoms of a hernia in a child
The main sign of a hernia is a bulge, which causes pain, usually in the epigastric region.
When the hernial sac is strangulated, the following symptoms are observed: severe pain at the site of the hernia, in severe cases - vomiting, fever, general weakness, bloating and peritoneal irritation.
The hernia is very difficult to reduce inside; touching it causes pain. In some cases, a hernia occurs without symptoms and is detected only when the child is examined by a doctor.
Increased pain is possible after eating, sudden movements, straining, and physical activity. Digestive disorders are often observed: belching, nausea, constipation, heartburn.
Causes of hernia
The causes of white line hernia in children are usually congenital. The main reason is congenital weakness of connective tissues. Other reasons include gender (hernia occurs more often in boys), obesity, constipation, ascites, chronic bronchitis and whooping cough, postoperative scars, etc.

Types of hernia and stages of its development
Depending on the location of the hernia in relation to the navel, several types of hernia of the white line are distinguished:
- supra-umbilical;
- subumbilical;
- peri-umbilical.
There are three main stages of hernia development:
- preperitoneal lipoma - protrusion of subperitoneal fat.
- the initial stage is the appearance of a hernial sac, into which the internal organs begin to fall out.
- formed hernia - divergence of the rectus muscles and prolapse of certain sections of the walls of the small intestine into the pouch.
Diagnosis of hernia
 A complete diagnosis of white line hernia will help to detect the disease in a timely manner and effectively treat it. Examination of the abdomen is carried out in a horizontal and vertical position of the patient with tense and relaxed muscles of the abdominal wall.
A complete diagnosis of white line hernia will help to detect the disease in a timely manner and effectively treat it. Examination of the abdomen is carried out in a horizontal and vertical position of the patient with tense and relaxed muscles of the abdominal wall.
The following methods are used to diagnose the disease:
- examination of the patient;
- interview and history taking;
- auscultation and palpation of the hernia;
- X-ray examination of the stomach;
- gastroscopy;
- urine and blood tests;
- MRI and CT scan of hernia (in difficult situations).
Differential diagnosis of white line hernia is usually carried out for the following diseases:
- cholecystitis;
- pancreatitis;
- stomach ulcer;
- tumor metastases to the omentum.
Hernia treatment

Photo: special bandage for a child
After making a diagnosis, the doctor chooses a method of treating the hernia. The most effective method is surgery. If the hernia is not removed in time, there is a risk of complications of the hernia and its further development. Activities such as massage for a hernia, wearing a bandage, etc. can only slow down the development of a hernia, but not eliminate the disease.
Contraindications to surgery are severe illness, the presence of infections in the body and the irreducibility of the hernia. In the presence of these contraindications, it is necessary to prevent the hernia from increasing in size. To do this, the child must wear a special bandage.
Surgical removal of a hernia – hernioplasty. The operation is usually performed under general anesthesia. The main types of operations: plastic surgery with local tissues (tension) and hernia repair using an endoprosthesis (non-tension).
Hernioplasty using your own tissue is performed to remove small hernias. In this case, the hernia is removed using continuous purse-string sutures. Tension hernioplasty can cause a recurrence of the hernia, since the sutures may not withstand heavy loads and cut through.
Hernioplasty using an endoprosthesis is usually performed to remove small and medium-sized hernias. This is the most effective surgical method for treating a hernia. Modern endoprostheses are characterized by high reliability and elasticity, without limiting the mobility of the abdominal wall.
The use of an endoprosthesis provides the following advantages compared to tension plastic surgery:
- painlessness. Typically, patients do not need to take pain medications after surgery.
- short rehabilitation period. The operation lasts about an hour, and the little patient can be discharged the next day. In some cases, he may remain in the hospital for a couple more days.
- low risk of relapse. The probability of relapse after using this method is no more than 1%, whereas when using tension plasty it is 20-40%.
Diet for hernia

When preparing a child for surgery, you should feed him dishes made from vegetables, cereals, rice, fruits, fish, egg whites, low-fat cheese, etc. It is necessary to exclude spicy and fatty foods, including spices, from the diet.
To speed up postoperative rehabilitation, the doctor prescribes a special diet rich in fruit and vegetable juices, cereals, and purees. However, it is not recommended to overuse fiber to avoid colic and flatulence. The child should also be given calcium, vitamins B and C after surgery.
In the postoperative period, it is extremely undesirable to consume foods that contribute to the development of constipation and gas formation.
Complications of hernia
The main complication of a hernia of the white line of the abdomen is its strangulation, in which the hernial contents are suddenly compressed in the hernial orifice.
If a hernia is strangulated, the child undergoes emergency surgery, which may involve large volumes of resection. The main symptoms of strangulation are vomiting, nausea, severe abdominal pain, inability to reduce the hernia, and the presence of blood in the stool.
Another complication of a hernia of the white line of the abdomen is the irreducibility of the hernia. In this case, the contents of the hernia are connected to the walls of the hernial sac.
In addition, injury and inflammation of the internal organ located in the hernial sac, as well as intestinal obstruction, are possible.
Hernia prevention
To prevent a hernia of the linea alba in infants, regular bowel movements should be performed. You should also ensure that the baby does not overeat and that his intestines work reliably.
For children aged 5-10 years, moderate physical exercise is an effective prevention of hernia formation.
It is necessary to regularly take the child for routine examinations to the doctor and accustom the child to moderate hardening.
In conclusion, it should be noted that a hernia of the linea alba in children can only be eliminated through surgery. It is very important to carry out diagnosis and surgery in a timely manner, otherwise complications are possible, first of all, strangulation of the hernia. But even after the operation, careful adherence to all doctor’s recommendations is necessary to prevent relapses.
SHARE WITH OTHERS IF YOU LIKED THIS ARTICLE



